

A fork in my 'cancer journey'--colon cancer markers
By Howard Wolinsky
I have been focused on prostate cancer since I was diagnosed 12 years ago. But I recently expanded my concerns to colon cancer, the third most common cancer in men and women, as a result of participating in a study on DNA and prostate cancer.
Colon cancer actually has been a risk for me since my mother Edith died at age 66 in 1988 from a melange of liver and spine metastases from primary breast and colon cancers. She also had uterine and skin cancer.

She died a horrible death. I remember her telling me: “I’d like to die now, but I don’t know how.”
Her situation haunted me. I had a recurrent nightmare of her calling me from her home in LA and asking me to come to help her. So I inexplicably set off on an ultra-marathon, running from Chicago to the San Fernando Valley. I got there too late. I was sweating and gasping for breath—in my dream.
It sounded like she had Lynch syndrome, a mix of cancers. But we’ll never know because she never had a genetic test let alone a colonoscopy. Symptoms from colon cancer, including diarrhea, eventually resulted in the diagnosis of colon cancer.
That diagnosis led to her three sons and one daughter starting on regular colonoscopies every five years rather than the 10-year intervals advised for most of you.
I have been recommending that all of my fellow prostate cancer patients undergo a free genetic test through the PROMISE registry (Prostate Cancer Registry of Outcomes and Germline Mutations For Improved Survival and Treatment Effectiveness), a collaboration between investigators at the University of Washington in Seattle and Johns Hopkins in Baltimore, studying how genetic variants can affect prostate cancer outcomes. (The study so far is only on Americans. But that may change.)
(My PROMISE results)
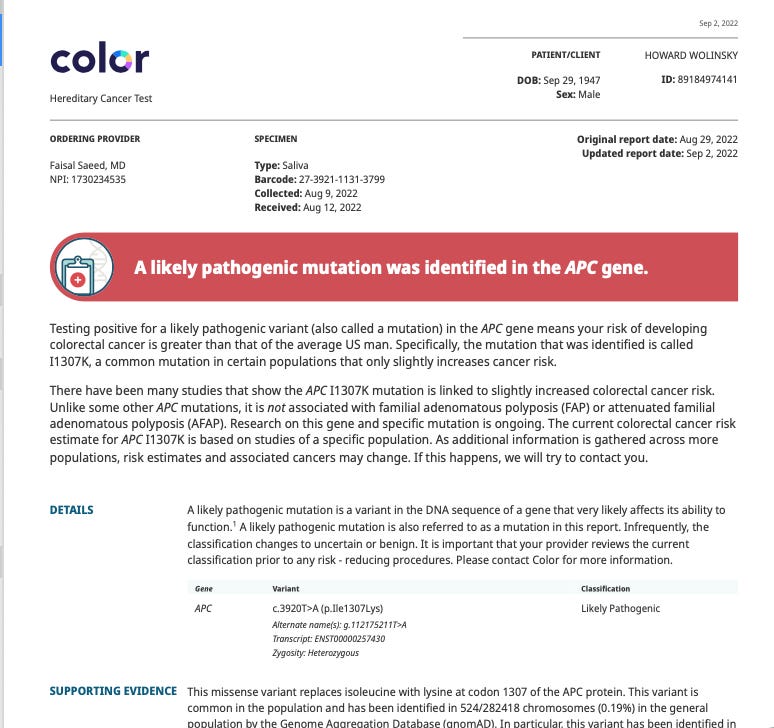
I took the Kool-Aid and registered for the PROMISE trial. No markers for prostate cancer were found. But there was a common marker for a low-risk colon cancer, APC, often found in Ashkenazi Jews (my peeps).
I told my sons and my brothers and my sister about the colon findings. It turns out that my younger sister, who had been diagnosed with breast cancer about five years ago, underwent DNA tests. She had the same APC gene for colon cancer but did not mention it to the rest of us. She did tell me back then that testing had ruled out Lynch syndrome.
One of my brothers got DNA tested through the PROMISE study and found he also had the APC colon variant. My remaining brother is weighing his options.
Read more in my column in Medpage this week: https://www.medpagetoday.com/special-reports/apatientsjourney/101619 and also read about my detour to the hospital with a bowel blockage at
Tick. Tock. Still time to answer the AS survey?
Active Surveillance Patients International, AnCan Virtual Support Group for Active Surveillance, Prostate Cancer Support Canada, and The Active Surveillor newsletter are asking you to participate in a survey on patient attitudes toward Active Surveillance,
To participate in the survey, click here: https://www.surveymonkey.com/r/W69XXDS
Please help us out. The survey closes Nov. 15. It takes five minutes and will impact how patients like us are treated.
The survey is open to patients on AS for low-risk Gleason 6 prostate cancer to favorable intermediate-risk prostate cancer as well as those who have moved on to treatment,
Data will be used to inform policymakers, guideline writers, and clinicians about the “patient voice” on key issues.
For example: Will renaming Gleason 6 lesions as noncancerous reduce mental distress and financial toxicity in patients on AS? Should U.S. guideline writers, as their European counterparts did last year? favor safer transperineal biopsies vs. transrectal biopsies that can cause sepsis and other infections?
Subscribed
Moving AS to the next level
By Howard Wolinsky
The Active Surveillance Coalition, a collaboration of leading support groups for active surveillance (AS) for prostate cancer, is sponsoring a webinar at 9 a.m. Vancouver/12 p.m. New York/5 p.m. London/6 p.m. Amsterdam on Thursday, Nov. 17 to discuss how we can move the needle on AS, close monitoring of prostate cancer.
AS leaders from Sweden, Holland, the United Kingdom, and the state of Michigan’s will share their “secret sauce” for reaching AS rates of near 90% and above.
The free webinar is entitled “Moving AS to the next level: Can we help more patients?”
Register here: https://bit.ly/ASnextlevel

The United States has lagged behind other wealthy countries in AS acceptance though the approach started here and in Canada in the late 1990s. AS uptake with AS finally reached a majority of 60% in 2021. The American Urological Association in 2022 set a new goal of 80% In 2010, only 6% of patients qualified for AS opted for this approach.
Several European countries and the state of Michigan’s MUSIC (Michigan Urological Surgery Improvement Collaborative) program have reached AS uptakes of around 90% or higher.
Panel members will present their stories followed by a discussion and a Q&A involving the audience.
Sign my petition to phase out transrectal biopsies. Read why: https://chng.it/7bQsWSfK Once we hit 1,000 signatures, we should begin letting Congress, Medicare, and the American Urological Association know. Please make no donations. This effort requires your signatures, not your money—at this point.
Rrparmer
12:31 PM (59 minutes ago)
to me
First Howard. Glad you survived blockage and hope your wife is doing better. Observations from reading your hospital stay piece:
1) Communication and timeliness are the Achilles heel of hospital stays even with short staffing. Just like in my first responder mountain rescue team (see below).
2) Most big (or small) hospital problems come from miscommunication or timeliness rather than performance or expertise issues.
Shit happens when verbal or written communication is off (re: failure to have someone else check your knots in mountain rescue or failure to listen or read shift nurse or doctor notes carefully)
3) Always have a patient advocate with you in hospital in any situation where critical decision making (i.e. surgery or not). Poor folks often do not.
A wise 64 year old Irish nurse told me this last Christmas Day while removing my catheter at home from aftermath of knee replacement. She also recommended pot (edible or inhaled) as alternative to opioid pill. Informed me this advice had to be off the record. She was right! It worked.
Finally, I had to convince my UCSF Dr. Shinohara NOT to give me another biopsy and instead monitor my PSA every 3 months and to do transperineal In past year my PSA jumped from 7.45 to 12 then back down to 10 which it has stayed at for 2 more tests. His rationale for biopsy. There was more cancer (no lesions) in last biopsy by specimen volume (highest 33% lowest 3% of 12 taken). Mine for not. I have been Gleason 3+3 for 14 years & though volume of carcinoma is increasing slowly I don’t feel I need another biopsy 18 months later.
Cheers, stay well
“water polo” Rick Parmer, Petaluma, CA