

European quality of life study: Anxiety and the uncertainties of Active Surveillance
Part 2 of a series on 'anxious surveillance'
(By Howard Wolinsky
A large European study shows that even Active Surveillance patients with low Gleason 6 scores facing an extremely low risk of dying from prostate cancer, are grappling with emotional distress (anxiety/depression/stress).
“Active surveillance seems to be associated with higher levels of depression or anxiety than treatments such as radical prostatectomy and radiotherapy. This may be related to the long-term worry that can be brought by regular testing, and the fact that treatment decisions may still have to be made,” according to EUOPROMS 2, a survey of more than 5,5000 patients from 32 countries, including the U.S. and Canada.
Anxious surveillance is no secret to many patients (about 50% of you who read TheActiveSurveillor.com) even though we avoid the risks of incontinence and sexual dysfunction from aggressive treatment. Many of us experience anxiety while waiting for results from prostate-specific antigen (PSA) blood tests, magnetic resonance imaging and biopsies and around the time of visits to the urologist.
However, urologists and researchers often have overlooked or downplayed anxiety. And the American Urological Association and American Society for Radiation Oncology, unlike most other medical organizations, don’t recommend screening cancer patients for emotional distress.

Europa UOMO, an association of more than 20 national advocacy groups for prostate cancer patients in Europe, presented its findings on quality of life earlier this year.
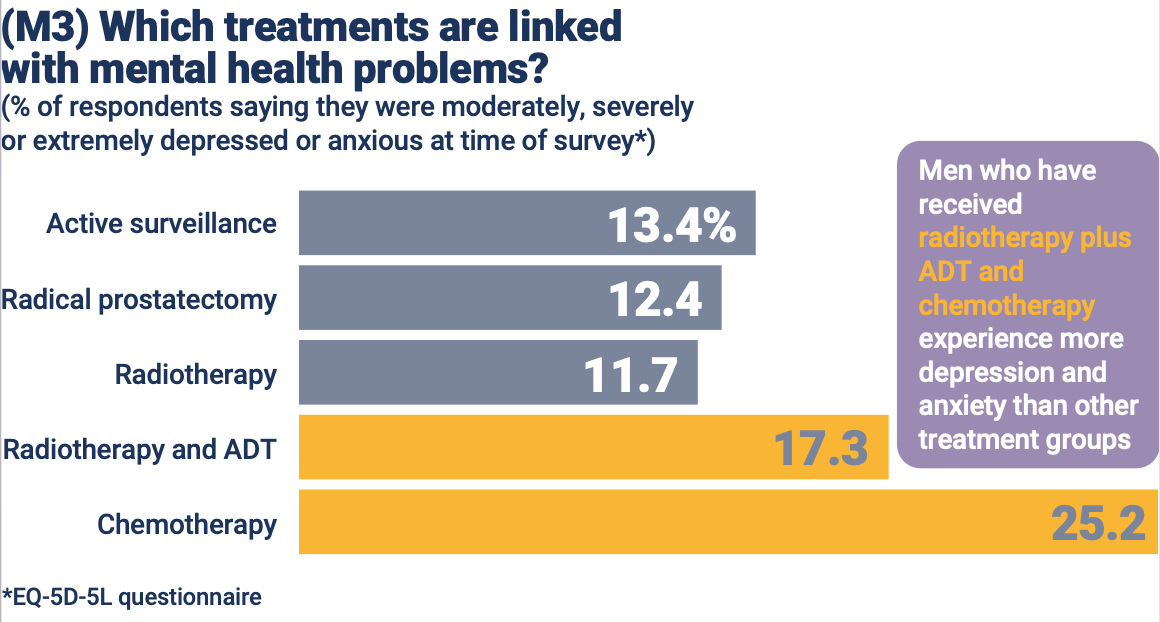
Overall, the researchers found 42% of men treated for prostate cancer say they are anxious or depressed to some degree—lower than the more than 50% we found in our survey but not far off. Problems seem to get worse the more advanced the cancer, becomes, when men are more likely to be receiving ADT (androgen-deprivation therapy) and chemotherapy, researchers said.
(The full EUPROMS study is available here: https://www.europa-uomo.org/wp-content/uploads/2023/08/EUPROMS_booklet_English_24Feb23.pdf)
Still, some patients with Gleason 6 (Grade Group 1) scores find their anxiety levels are so high they opt for radical prostatectomies or radiation. Some—not all—urologists and radiation oncologists are willing to provide aggressive therapy to Gleason 6 patients to overcome anxiety.
***
Health psychologist Lara Bellardita, Ph.D., Psy.D, has been researching the psychological issues faced by men on active surveillance (AS). She is affiliated with the National Cancer Institute in Milan, where she has been studying how to keep men experiencing anxious surveillance to adjust and stay out of the OR and the radiation suite.
Overcoming ‘anxious surveillance,’ staying on active surveillance

We call it “anxious surveillance” because some guys on AS can experience anxiety around the time when they are scheduled to undergo a urology exam, a PSA, biopsy, MRI, or when we wait for the results. An AnCan survey in 2021 of 165 men on AS found that 30% of men experience anxious surveillance, often because of pressure from spouses and family. Even the…
She contends that a couple of counseling sessions can do the trick to help men overcome anxiety they experience from choosing AS over active treatment or staying on AS and waiting for results from testing.
Dr. Bellardita stresses: “Prostatectomy is not a solution for anxiety.”
***
Research at Memorial Sloan Kettering (MSK) Cancer Center in New York showed that after about two years on AS, most patients make their adjustments.
In this study, soon after diagnosis, one in three men reported anxiety. After 5 years, one in five did. After 10 years, about one in 10 report anxiety. The tincture of time reduces anxiety levels.
The MSK study showed that men considering AS may have some initial worry but they'll adjust to AS rapidly.
Andrew Vickers, PhD, a biostatistician at MSK, said, "Our conclusion is that when men are going on active surveillance you should say something like, 'You may feel anxious. That's perfectly normal. Quite a few men feel a little bit anxious in the first year or so but it goes away over time. Most men sort of get used to it and they get comfortable with it. And anxiety is not really a major problem in the long term for people in active surveillance.'"
(Vickers described being at an international meeting where a Dutch doctor said in his experience some patients are too anxious to go on AS. The Dutch clinician said such patients simply ought to undergo radical prostatectomy -- without being offered AS. Yikes. That’s harsh.)
***
The EUPROMS study found that men with more advanced prostate cancer experience roughly equal levels of anxiety in the first and second line of treatment, and anxiety and depression tend to diminish after treatment ends.
Researchers said: “But a recurrence can affect mental health a great deal. Almost half of the respondents who had a recurrence rate the effect on their mental health as six or more on a scale of one to ten – in other words, it had a significant effect.”
EUPROMS found clear advantages to AS compared to aggressive treatment in terms of quality of life.
Some men on AS have urinary incontinence and erectile problems. You can’t always blame prostates and aggressive treatment. Aging can play a role.
My friend Gerald Chodak, MD, the late urologist whose research at UChicago lead to AS becoming a strategy in the 1990s, told me when I was the medical editor at the Chicago Sun-Times that too many surgeons did not screen their patients for erectile and continence problems before surgery. So surgery was blamed for problems it may not have caused.
Uomo results:
However, researchers said comparing the surgery figure with active surveillance shows that surgery doubles the rate of incontinence.

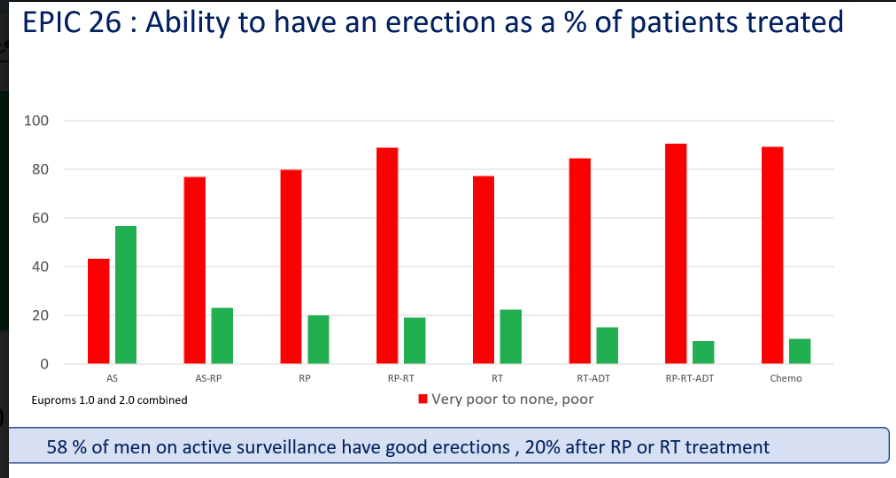
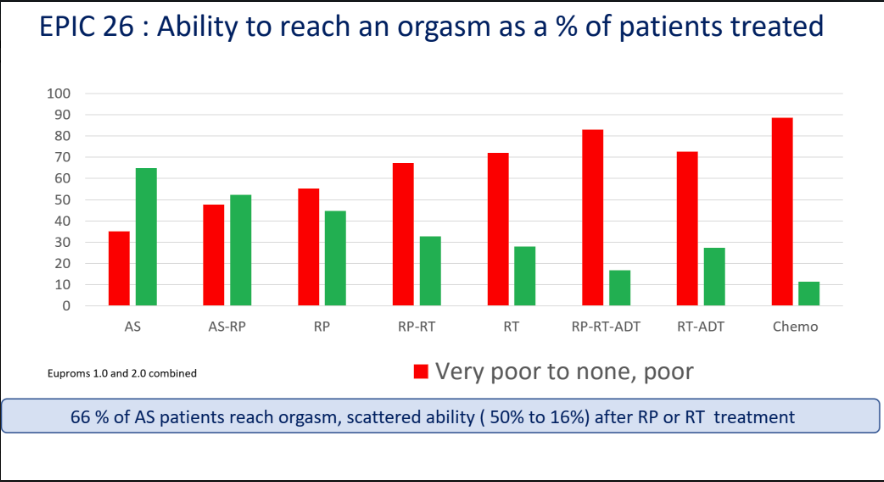
As to sexual function, not surprisingly men on AS fared best. That’s one of the points of AS, right? Same with retaining urinary continence.
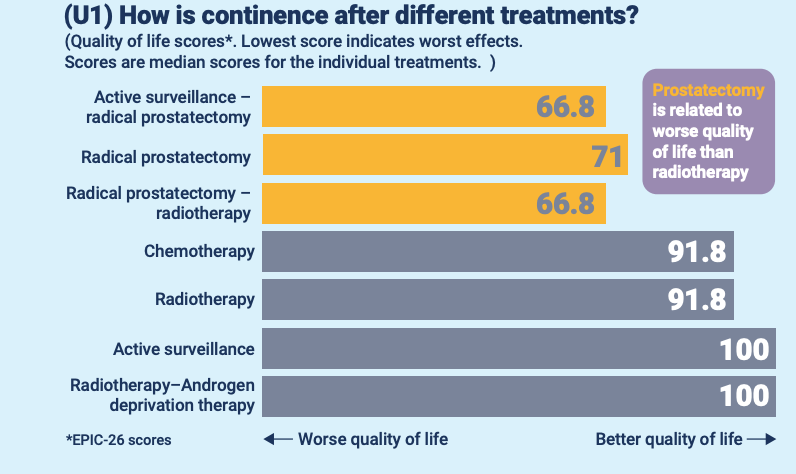
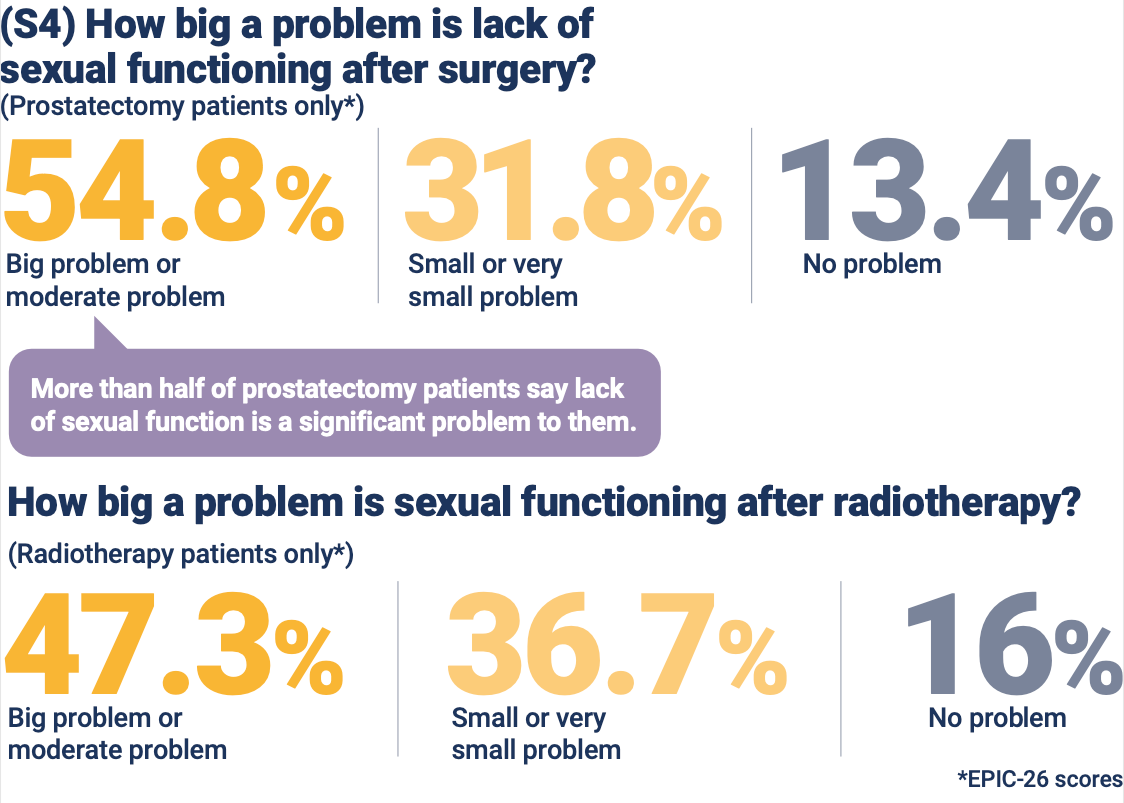
Researchers noted: “Sexual functioning seems to be a slightly less significant problem after radiotherapy: 47.3% of men who have had radiotherapy have significant problems compared with 54.8% for prostatectomy.”
Surprising to me, how few respondents—mainly from Europe—try the Little Blue Pill (Viagra) and the like:


In the U.S. 40% of men with Gleason 6 (Grade Group 1) still opt for treatment rather than AS. Of men with low-risk Gleason 6, 10% or fewer pick treatment in Michigan, Sweden, the United Kingdom.
FYI, here’s a comparison of surgery and radiotherapy regarding sexual functioning:
EUPROMS researchers made these take-home points:
—Active surveillance should always be considered if it can be applied safely because overall it best protects quality of life. The contrast between active surveillance and other approaches is particularly clear in terms of incontinence and sexual function.
—Early detection of prostate cancer is of the utmost importance. The more advanced the prostate cancer at diagnosis, the worse the effects of treatment on quality of life. The research clearly shows that many symptoms that affect the quality of life are experienced more severely with treatments associated with more advanced prostate cancer.
—High-quality treatment and support are essential. The EUPROMS results show the severe effects that can come with treatment for prostate cancer. Men need all the expertise and experience they can get during treatment and after, with information and support at each stage of the journey. Every man with prostate cancer should be treated in a cancer center with multidisciplinary teams.
***
Editor’s note: This is the second in a series of articles on “anxious surveillance.” The first part covered how the pioneering Michigan Urological Surgery Improvement Collaborative (MUSIC) tackled anxiety in Active Surveillance:
MUSIC addresses Anxious Surveillance

By Howard Wolinsky Anxiety is so common in men on Active Surveillance (AS) for lower-risk prostate cancer that we have a name for it: Anxious Surveillance. It’s common: 55% of us experience it. 10% experience severe anxiety that can drive us to seek aggressive treatment, according to a survey of 450 men who are on or were on AS.
You’ve got questions? They’ve got answers.
By Howard Wolinsky
TheActiveSurveillor.com team of prostate cancer experts is answering your questions about Active Surveillance and lower-risk prostate cancer. These top docs will respond to your questions about pathology, urology, radiology, lifestyle, and sexuality.
Please send questions via email to mailto:pros8canswers@gmail.com
Keep the questions short and sweet. They should be of general interest. Sign with your real name, initials, where you live, and how long you have been on AS.
(We don’t offer medical advice. Go to your personal physicians for that.)
March Madness and Active Surveillance: Why not sign up?
By Howard Wolinsky
For the past three years,support group moderators Joe Gallo, Jim Schraidt, and I have run a special Active Surveillance support group for ZERO. Last year, our virtual support meeting drew 60 patients to talk about AS. By far, it was the biggest session of any at the annual ZERO Summit.
I’m hoping we can beat that record at 10 a.m. Central on March 12, 2024 as part of ZERO’s annual Summit.
I’ve set up the meeting and figured why not put out the word early.
It also will help in planning. If we get over 100 sign-ups, I’ll have to convert to a webinar so no one gets turned away.
So sign up now and join us in March. We’ll do a little one-on-one for about an hour.
Here’s the invitation:
Hi, all.
You are invited to a Zoom meeting.
When: Mar 12, 2024 10:00 AM Central Time (US and Canada)
Register in advance for this meeting:
https://us02web.zoom.us/meeting/register/tZUsfuqgrjIoG9AWf7voMhzT_UjdqbQQbQPA
After registering, you will receive a confirmation email containing information about joining the meeting.
Now a word from a subscriber
Thanks, Keith. I do what I can. And so do you:
Keith Holden is a physician sharing his advanced prostate cancer journey at “Prostate Cancer Secrets.” He talks about PSAnxiety, financial toxicity, and other topics of interest to all of us on this path. Check him out.

{kind=link}
Final word on free webinar
Join Sharsheret's annual Let's Talk About Men webinar open to all men and women, including those who carry genetic mutations such as BRCA, CHEK2, PALB2, etc. Doctors will discuss screening guidelines for cancers that affect men including prostate, colon and pancreatic cancers.
Men at elevated genetic risk for, or who have been diagnosed with, male breast cancer are invited to join the breakout room following the formal conclusion of the webinar

Registration:
https://sharsheret-org.givecloud.co/product/Menswebinar23/lets-talk-about-men-essential-screening-guidelines-every-man-should-know