

Ramping up for 'Active Surveillance 2025' webinar--hope you're coming to hear leaders in the field on Jan. 4
JP pays it forward to The Active Surveillor
By Howard Wolinsky
I set up the “AS ‘25” webinar in response to requests from paid subscribers who wanted a premium for their donations to help keep The Active Surveillor afloat.
I have always offered the same content to all subscribers—paid or unpaid. Many Substack newsletters is to send posts for paid subscribers only.
I can’t do that. There is news in this Substack that most patients don’t have access to anywhere else.
My goal was to keep readers informed about the latest in news on AS as well as offering articles about AS, profiles on patients, first-person columns, etc. It felt wrong to do it any other way,
I have nearly 2,000 subscribers since I started this newsletter in January 2002. Just under 300 pay for subscriptions to support my efforts to meet my motto: “Saving prostates daily.”
Unfortunately, I had to start asking for paid subscriptions. Almost immediately when I launched the newsletter, I found I was losing money, several thousand a year as I paid for software, tech tools, professional transcription of interviews, etc. Plus the U.S. Department of Treasury and Substack, the publisher, and its financial arm Stripe took a bite, skimming about 40% off the top.
It’s a Sisyphean task to keep this little publication going. I am writer, editor (sorry for the typos—I can’t afford an editor), marketer/publicist, subscription manager, chief cook and bottle washer.
There is constant churn among readers. People come and go as their diagnoses change. I was a newspaper reporter for 50 years and never appreciated what the circulation department or other departments did to keep us going. Please accept a belated apology.
Meanwhile, I have been touched by the generosity of readers in sharing their personal cancer journeys as well as digging into their wallets to help me out. A coouple loyal followers have purchased multiple annual subscriptions and donated them to pay for subscriptions for those who can’t pay themselves.
Some long-time readers have made the switch to paid ($80/year or $9/month) from unpaid. One reader offered part of his inheritance to fill any gap. I appreciate the offer, but I felt that wasn’t sustainable.
My Public TV plea here: You can help by getting a paid subscription here:
I have been touched by the supportive notes I have received from many readers.
Here’s one from JP, , 58, who has high-volume Gleason 6 (Grade Group 1) cancer.
He told me: “I have been following you for the past year since I formally joined the PCa club, and felt it was time I started paying for the good advice you have offered me.
(NOTE: No medical advice is intended, but I share my personal experience. I am not a medical professional.)
JP continued: “You don't know me, but I suspect you [know men like me]. I was diagnosed with the best cancer you can have on Halloween 2023. (I felt like Charlie Brown getting a rock!) Gleason 6. It's not even cancer, so I shouldn't have to worry about it too much!
“My wrinkle is that it's high volume, in basically 30% of the prostate.
“My urologist ordered genetic testing, and the results are a slightly above average score but not near the ‘bad’ threshold. My urologist suggested I start AS, and we agreed that while higher than average risk. AS was an acceptable treatment, but I would be ready to consider active treatment if scores move in the wrong direction. We're good, but the risks are as clear as mud!
“As background, I am a number- and fact-oriented analytic person who focuses on risk and probabilities in my decision-making.
“I am the youngest of 5 brothers with no family history of PCa until about 7 years ago. I never imagined PCa as an issue in my life until one of my brothers was diagnosed about seven years ago. Subsequently, 4 of us have been diagnosed, and my oldest brother died of a particularly nasty case in about 10 months. One dead, one seeds, one RALP (robotic-assisted laparoscopic prostatectomy). and me on AS.
“My family has become our own personal cancer cluster! I haven't found any research or models that help me out on this one! Any suggestions are welcome. I've just started thinking about the implications for my two sons and 10 male nephews. 80% hit rate in the prior generation is a Shit Sandwich. It's made me angry.
[Note: Female family members need not worry about prostate cancer. But sometimes, other cancers such as colon, ovarian, pancreas and breast can be tied in. JP plans to delve more into his cancer genetic inheritance.]
“I have found your newsletter very helpful, and it has helped me through the last year. The least I could do is start paying you for it and owe you for a prior year's subscription. I signed up for a monthly payment and am hoping to pay you back over time. If all goes well, you will be overpaid, which would signify a good thing for me.
“It's been cathartic to write. $9/month was well spent, and I'm looking forward to overpaying monthly for a long time.
“I thought about hitting delete rather than sending this, but F-it. I am a fan of yours and I paid my $9.
Thanks to JP and all others who will be attending. More than 150 have registered to date.
(Clockwise from upper left: Epstein, Helfand, Showalter, and Pavlovich.)
Speakers for “Active Surveillance 2025” include:
--Jonathan Epstein, MD, former chief pathologist at Johns Hopkins University School of Medicine, one of the world's leading pathologists. Epstein, now based in New York, will be making his first appearance before a patient audience in almost two years,
—Brian Helfand, MD, PhD, chief of urology at NorthShore University HealthSystem outside Chicago, an expert not only in prostate cancer but also in molecular biology.
—Christian Pavlovich, MD, who runs the Active Surveillance program at Johns Hopkins and recently co-authored a major study on diet.
—Timothy Showalter, MD, MPH, medical director of Artera AI, which has made news with its prostate test to help patients decide whether to go on AS.
Hope you’ll start the new year with us.
Sports world leading way in informing public about prostate cancer
By Howard Wolinsky
Last week, former ESPN NBA Insider Adrian '“woj” Wojnarowski revealed he was on Active Surveillance for low-risk prostate cancer.
Few high-profile people who develop low-risk prostate cancer share their stories publicly.
They can hide their cancers with the public being none the wiser.

It’s a different story for advanced prostate cancer. These men may not be able to “hide” their cancers because of physical changes from treatment and disease and because of hospitalizations.
Back in August Chicago Cubs Hall of Famer Ryne Sandberg said he was cancer free after radiation treatment for metastatic prostate cancer. He had
Sadly, he announced Tuesday that his cancer has returned and spread.
Sandberg had said in August that he was cancer-free, after radiation treatments for metastatic prostate cancer.
However, on Tuesday, he posted on Instagram that he had an update.
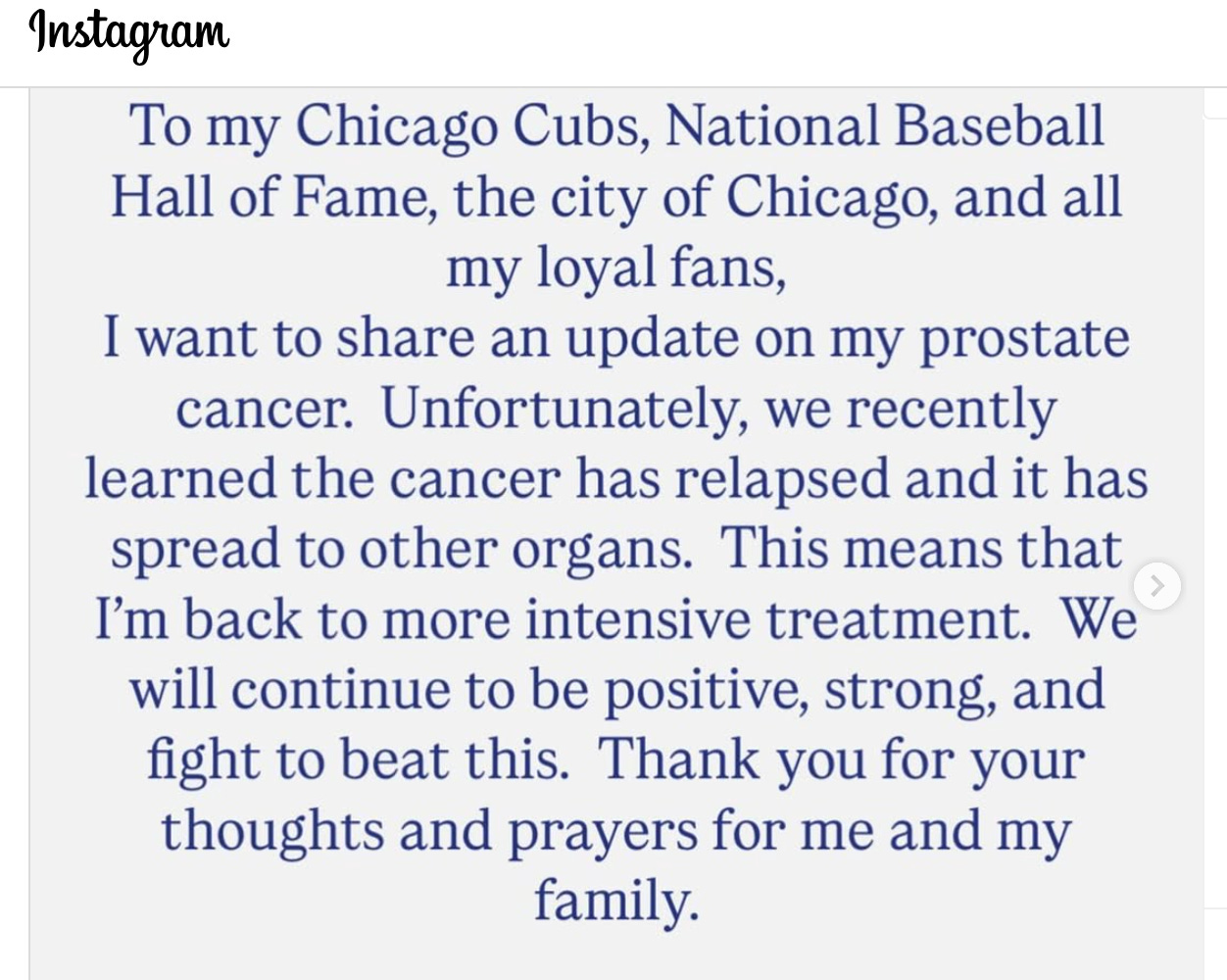
The Cubs honored the legend this summer with his own statue outside of Wrigley Field.
Sandberg was a 10-time All-Star during his 15 seasons for the Cubs from 1982 to 1997, amassing 282 home runs and 344 stolen bases. After his playing career, he served as manager of the Philadelphia Phillies from 2013 to 2015, going 119-159.
Sandberg won the National League MVP in 1984, the year the Cubs won a division title. He led the league in triples and runs scored that season, while hitting .314 with 19 home runs.
In 1990, Sandberg hit 40 home runs, becoming just the third primary second baseman to reach the 40-homer plateau. He was elected to the National Baseball Hall of Fame in 2005.
Thanks to Ryno and Woj for sharing their very different prostate cancer stories and for educating the public on the most common cancer in American men.
Correct, Jeff, if you can afford it with future replete with uncertainty for all, do it! Have it from an unreliable source at the Pearly Gates, each of us WILL be asked were we a sustaining member of The Active Surveillor.
Dr. Vorstman, yes, where is the discussion regarding PI RADS 4/5 and low risk upon biopsy; is it more common than one suspects? Continue to write to force experts or not alike "out of the closet" on issues you raise.
Thanks for the support, Jeff. Good to know I can outclass Paramount. Where do I stand in view of Apple, Netflix, or Hulu.
You're citing the monthly rate for the newsletter. The annual rate is cheaper.
My 2 cents.
Howard