

In the future: AI in 'blood-based biopsy' for Active Surveillance patients
By Howard Wolinsky
We’ve been hearing a lot lately about AI (artificial intelligence). Brace yourself. We’ll likely be hearing more and more as time goes on. This isn’t just a fad.
With AI, millions of files are fed into “machine learning” systems to train them on how to read multiparametric magnetic resonance imaging (MRI) scans. AI reads of MRIs are good and getting better.
AI is making inroads in reading pathology slides, too. I recently ran a Q&A on ArteraAI, which uses a patient's existing pathology slides and digitizes them for the AI program. The AI then combines this information to predict whether a patient will benefit from a particular therapy and estimate long-term outcomes.
Today’s AI story is applying a similar approach to a “blood-based biopsy technology" looking at genomic data developed by Immunis.AI, a Detroit area startup. Immunis.AI extracts information from a patient's immune system to detect prostate cancer and determine whether there is a risk that the cancer is aggressive. Based on this risk score, patients and providers can make better decisions about entering, continuing, or stopping an active surveillance protocol.
Watch out, pathologists and urologists. These are early days, but it’s worthwhile to keep an eye on companies like Immunis.AI, especially because patients like most of us on Active Surveillance protocols are its initial market.
Their idea is to disrupt the market for prostate-specific antigen (PSA) testing, MRIs, and biopsies.

(Kirk Wojno, MD, Immunis.AI’s chief medical officer.)
Following is a Q&A with pathologist Kirk Wojno, MD, Immunis.AI’s chief medical officer.
What got Immunis.AI interested in prostate cancer active surveillance?
Our scientific founder, Dr. Amin Kassis from Harvard Medical School, was studying the gene expression profiles of immune cells to investigate how to evaluate patients with a personalized medicine approach.
What he didn’t realize at the time was that he was studying within the immuno-oncology space before it became popular like it is today. In doing this, he was figuring out how to identify when cancer transitions from indolent to aggressive, an area that hasn’t gotten much attention.
Prostate cancer is at the forefront of deciding what active surveillance is and how it should be used, but prostate cancer active surveillance still has a high unmet need and doesn’t get much attention. In the developing cancer treatment landscape, this will become increasingly important as more patients opt for active surveillance for indolent cancers. Patients on active surveillance for prostate cancer have risen more than 30% in the last ten years. As opposed to and not to be confused with watchful waiting, active surveillance is a first-line treatment modality for cancer when used correctly. Immunis.AI is interested in making active surveillance decisions easier and better; we want patients to feel comfortable entering and staying on active surveillance for their indolent cancer and that if and when a cancer becomes clinically significant, we can detect that change early when treatment is possible.
What do you mean when you say active surveillance compliance is only 32%?
If a patient has gone on an active surveillance protocol and didn’t follow it, whether low- or high-intensity, the patient is not complying with their active surveillance recommendations. These active surveillance protocols are not uniform across medical practices and differ in the number and timing of follow-up tests. Whether a patient is supposed to have a biopsy at 12 months, 18 months, or 24 months, if they have missed the biopsy or decided not to have one, they would be part of the 68% that are not compliant with their active surveillance protocol. Active surveillance is delayed therapy, where the intent remains to cure. Active surveillance may be able to delay definitive treatment for someone’s entire life because their cancer will never become clinically significant, but patients have to have careful monitoring during that time for it to be successful. Forgoing biopsies and ignoring the cancer may result in its progression to a point where it is no longer easily treatable.
What is wrong with the current system of active surveillance?
PSA tests and up-and-coming liquid biopsies often rely on circulating tumor cells or cell-free DNA that are only readily detectable at later stages of the disease. These tests fall short in their ability to detect the earlier stage of cancer when it transitions from indolent to aggressive and clinically significant.
Traditional prostate needle biopsies are invasive and can miss up to 25% of clinically relevant disease.
After many years of prostate biopsies, patients often feel like a pincushion and don’t want further biopsies. Current screening techniques also fail to provide valuable information about the risk of cancer progression, which can inform decisions regarding active surveillance.
Something I’ve seen as a pathologist, and what many people don’t know, is that some of the very high-grade aggressive cancers don’t make elevated amounts of PSA. I’ve seen terrible cancers with very low PSA levels, so we need something better. (Emphasis added.)
Because our technology evaluates the immune signature instead of tissue or circulating tumor cells, we can detect indolent prostate cancer and the risk of that cancer becoming aggressive down the road, which is heavily dependent on the immune response to the presence of cancer.
What role does the immune system play in indolent and aggressive prostate cancer?
The difference between indolent and aggressive cancers comes down to how well-controlled the cancer is by the immune system. In low-grade, indolent cancers, the immune system does a great job of keeping that tumor at bay, preventing it from growing and spreading throughout the body. But when there’s some disruption to the immune system, like a person has stressors in their life or their environmental conditions change, their immune surveillance system changes and can weaken. Once the immune system is weakened, tumors can escape the immune system. These cancers are smart, and once they punch through our immune surveillance system and start growing, they become much more aggressive and clinically significant. Because of this, the immune system can serve as a reliable indicator of cancer’s aggressiveness.
How does Immunis.AI’s technology work?
Our technology uses an immuno-transcriptomic approach to harness the power of the immune system to detect and stratify cancer. The test creates an immune profile specific to each patient to get a real-time view of the immune system and gain information about the presence and severity of prostate cancer.
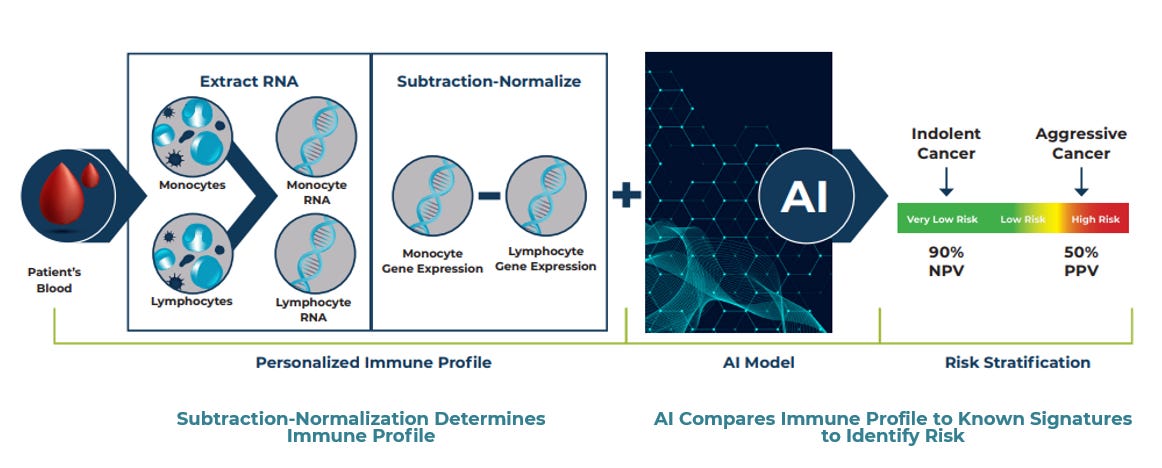
Each person’s immune profile can be assessed by looking at two types of immune cells – monocytes and lymphocytes. RNA from these two cell types is extracted, and gene expression levels are calculated from the RNA expression levels. Then, the patient’s immune profile is created by subtracting lymphocyte gene expression levels from monocyte gene expression levels on a gene-by-gene basis using a process called subtraction-normalization. We have identified dozens of genes that make up the immune profile. An important feature of this immune profile is that the patient can serve as their own control. The two different cell types, monocytes and lymphocytes, are cells from the innate and adaptive immune systems.
These two cell types have completely different functions and respond differently to cancer. For each gene, the gene expression in one of these two cell types serves as the control for normal gene expression levels, while the other cell type interrogates the disease process. This will be different for each patient, allowing us to create a personalized immune profile specific to each patient. Unlike other liquid biopsies, which choose a few reference genes to compare to, our technology considers all the dynamic fluctuations in gene expression within a person. It allows the patient to serve as their own control, eliminating the confounding effects of patient-to-patient variability in gene expression levels. After the immune profile is characterized, the subtraction-normalized immune profile of each patient is evaluated against known immune signatures for indolent or aggressive prostate cancer using AI predictive modeling. Based on the similarity of each patient’s immune profile to these known immune signatures, the model produces an individualized risk score for each patient, categorizing them into one of three groups: very low-risk, low-risk and high-risk for developing clinically significant prostate cancer.
What does Immunis.AI’s technology add to the active surveillance process?
Our technology allows patients to be quickly and painlessly monitored at their active surveillance appointment with a simple blood-based test. Instead of having an invasive biopsy, MRI, or possibly inaccurate PSA test, patients will be tested with our immuno-transcriptomic technology. At every appointment, our test will provide the patient with an updated risk score that allows them and their provider to determine and track their risk of developing aggressive cancer over time and make decisions to begin, continue, or stop an active surveillance protocol.
How are the results presented to patients?
The output of our technology is a risk score, which puts the patient into one of three groups: very low-risk, low-risk (average risk), or high-risk for developing clinically significant prostate cancer. Once cancer is identified, the risk score will enable providers and patients to decide to enter an active surveillance protocol or pursue definitive therapy at their first appointment. These groups are defined so that a patient in the high-risk category has a positive predictive value high enough that they are willing to forgo active surveillance and move to definitive therapy. For a patient in the low-risk category, the assumption is that they have the same risk today as a patient with indolent cancer or when they entered active surveillance, and they can start or remain on a standard active surveillance protocol. For patients at very low risk, the chance of having clinically significant prostate cancer is very low, allowing them to go on a relaxed active surveillance protocol. Depending on the specific protocol, those who enter active surveillance will typically be monitored at least once a year to provide an updated risk score to inform decisions on continuing or stopping active surveillance.
How is it different from other liquid biopsy technologies, which perform poorly in identifying early-stage prostate cancer? Is your technology specifically of value to low-risk patients?
Most technologies detect cell-free DNA released from tumor cells. There must be enough tumor cells to release enough DNA to detect the cancer via blood tests. This makes the detection of early-stage prostate cancer difficult, as the tumor is not large enough to release large amounts of cell-free DNA. Unlike others, our test does not rely on cell-free DNA or circulating tumor cells. The immune system responds to cancer no matter how small it is. So even for early-stage indolent cancers, the immune system knows you have cancer and reacts in a certain way. The reaction of the immune system to aggressive cancers looks different as well. By looking at the immune profile, our test can detect the immune system’s response to cancer in real-time. This gives a snapshot of the immune system that can inform whether your cancer is under control by the immune system and indolent or has escaped the immune system and is potentially clinically significant. Because of this, our technology is especially equipped for the active surveillance population where most patients have localized, low-grade, low-risk cancers that cannot be easily detected by other tests.
What role does AI play in your technology?
AI’s main role in our technology has been in developing the immune signatures of indolent and aggressive prostate cancers. To do this, we looked at very large cohorts of prostate cancer patients and used AI to tease out the signature. We partnered with sophisticated mathematicians and statistical analysts at InfiniaML, a spin-out from Duke University, to use an iterative machine learning approach to discover the important immune system genes. These data were used to train our model and develop the validated immune signatures of indolent and aggressive prostate cancer that our test uses today.
Because of the non-invasive blood-based approach, these immune signatures are comprehensive and help to capture the tumor’s heterogeneity, something a prostate needle biopsy doesn’t do. There are over 64 different morphologic patterns of prostate cancer. Various immune factors may be over or under-expressed for each cancer, but by looking at the full immune profile for each patient, we can use AI to compare the patient’s individualized profile to these known immune signatures, regardless of the patient’s tumor type. Once the patient’s immune profile is compared to the known immune signatures via AI, we can provide them with a sophisticated, actionable report on their cancer in the form of a risk score.
What studies have you done on patients with this technology?
We have conducted three large prospective clinical studies - some of the largest of their kind ever performed in prostate cancer diagnostics. Our second of three large prostate cancer studies will be published in the Journal of Urology soon. This is a pivotal paper where we have defined the signature required to detect indolent and aggressive prostate cancer, and we have optimized our technology to answer these difficult clinical questions:
When should a patient be on active surveillance? When should a patient come off active surveillance?
Our technology was put to the test in this paper by evaluating a cohort of patients who have confirmed prostate cancer via biopsy. Later this year, we will publish results from our third large, multi-year study where we have evaluated the technology in an intended-use population, men on active surveillance. The study has 19 active clinical sites across the country, where we’ve collected these patients and carefully characterized them, following them long-term for up to 10 years. In this study, these men are being monitored with our blood test annually because we want to demonstrate the utility of our test in tracking the risk of clinically significant prostate cancer over time.
We are very excited about the results, and our preliminary data show that each specific patient will have a certain set of genes out of the signature that are important, which we will use to track changes in their cancer aggressiveness over time. With serial monitoring, these patients and providers are using our test to help decide whether it is safe to stay on active surveillance over time.
Will this technology also be used for prostate cancer screening like PSA levels?
Our technology will not be a screening tool for asymptomatic patient populations. Rather, a urologist would order our test for patients with suspected or confirmed prostate cancer who are considering active surveillance or are already on active surveillance. The patient would have their blood drawn and sent to our lab for testing. The results would be returned to the physician in 36-96 hours. This risk score will allow the patient and provider to decide whether to enter, continue, or stop an active surveillance protocol. If the patient’s risk score for aggressive cancer remains unchanged, they will remain on active surveillance and return for follow-up tests.
Are you looking beyond prostate cancer?
Our clinical studies thus far have focused on the prostate cancer active surveillance market. We have already begun clinical studies in two other urological cancers, kidney and bladder, and we expect to publish results in those markets in the next couple of years.
How will the test be marketed?
The test will be offered as a Laboratory Developed Test (LDT), which means urologists would collect the sample and ship it to our laboratory, where we would conduct the test. We plan to introduce the test as Research Use Only (RUO) to allow key opinion leaders to use and evaluate the test. Following the RUO introduction, we will roll out the test to the rest of the clinical market. We anticipate this process to start in 2024 - 2025.
Kirk Wojno, MD, is the chief medical officer at Immunis.AI. He is a board-certified anatomic and clinical pathologist, who trained at The Johns Hopkins Hospital and holds subspecialty boards in clinical chemistry as well as having extensive experience running molecular diagnostic laboratories.
Large uro practice leader boosts AS as prom king in low-risk prostate cancer
By Howard Wolinsky
We know from data generated by the American Urological Association that about 60% of men with low-risk prostate cancer now opt for Active Surveillance, up from about 6% in 2010.
Now a leader in the Large Urology Group Practice Association (LUGPA), the private urology groups, told his urology colleagues that they need to keep on pushing for surveillance rather than aggressive treatment in men with low-risk prostate cancer.
“I think urology as a whole needs to continue to push that agenda in low-risk men who probably benefit most from avoiding some of the side effects of therapy,” David S. Morris, MD, FACS, told a session from the 2023 LUGPA Annual Meeting titled, “Best Practices for Active Surveillance.”
Morris is the president and co-director of the advanced therapeutics center and research departments at Urology Associates in Nashville, Tennessee.
“[In] the intermediate-risk men, it’s more of a shared decision-making model about delaying therapy vs aggressive upfront treatment. All our tools, including genomics and MRI enable us to do a better job of risk stratifying to have a more appropriate shared decision-making discussion.”
For video go to Urology Today.
You’ve got questions? They’ve got answers.
By Howard Wolinsky
TheActiveSurveillor.com panel of experts will answer your questions about Active Surveillance and lower-risk prostate cancer.
These top docs will respond to your questions about pathology, urology, radiology, and sex and surveillance.
Please send questions via email to mailto:pros8canswers@gmail.com
Keep the questions short and sweet. They should be of general interest. Sign with your real name, initials, where you live, how long you have been on AS. Whimsical signatures are preferred, like Nervous in Nebraska, or Anxious in Alberta.
(We cannot offer medical advice. Go to your personal physicians for that.)
Now a word from a subscriber
