

Incidence of PCa nipping at heels of BrCa. But BrCa wins race for research bucks.

By Howard Wolinsky
It happens every January.
The American Cancer Society (ACS), the largest non-government funder of cancer research in the USA, releases its estimates for incidence and deaths from all cancers in the coming year.
The 2025 ACS figures show the incidence of prostate cancer in recent years has been narrowing the gender gap with the incidence of breast cancer in women as the #1 cause of cancer by sex. PCa is breathing down the neck of BrCa, and soon could catch and surpass BCa.
Not that anyone is looking for bragging rights.
Ironically, the ACS reported last week that more women overall will be diagnosed with all cancers than men for the first time in more than 100 years.
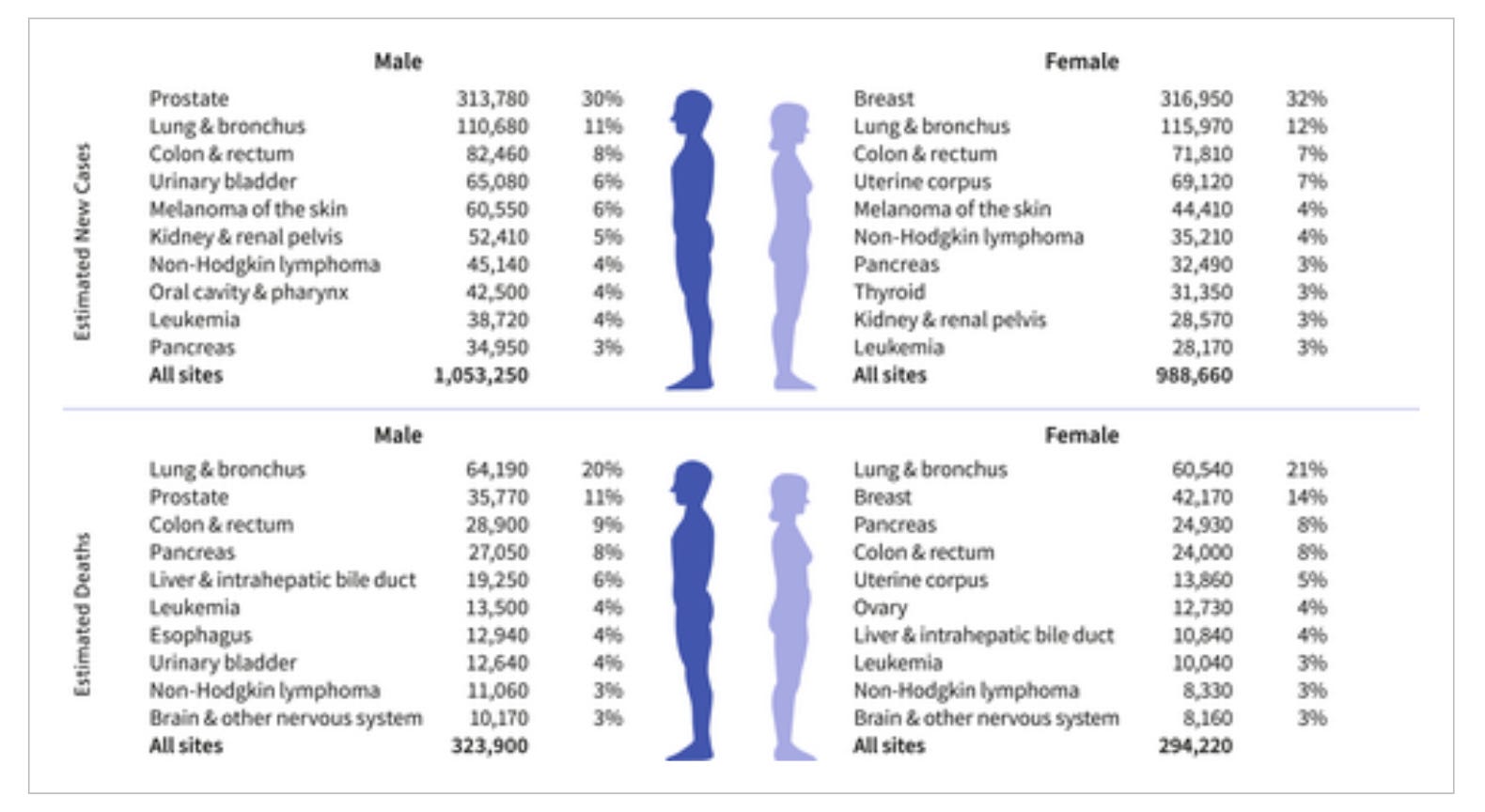
Among the findings projected for 2025:
—The incidence of prostate cancer is expected to crack 300,000 cases in 2025. ACS predicts there will be 313,780 new cases of prostate cancer this year.
Breast cancer is the most commonly diagnosed cancer in American women and prostate cancer the most common cancer in American men.
—The gap between new prostate cancer and new breast cancer cases this year will narrow to 3,170 cases. Last year, there were 11,710 more breast cancer cases than PCa cases.
—Lung cancer is projected to be the leading cause of cancer death in both men and women in 2025. Breast cancer with 42,120 deaths and prostate with 35,770 are projected tostill be ranked second in mortality by sex.
—Incidence rates continue to climb for common cancers, including breast (female), prostate (steepest increase at 3% per year from 2014-2021), pancreatic, uterine corpus, melanoma (female), liver (female), and oral cancers associated with the human papillomavirus.
—Black people are twice as likely to die of prostate, stomach, and uterine corpus cancers compared to White people and 50% more likely to die from cervical cancer, which is preventable.
ACS said there is an “increasing incidence for many cancer types, especially among women and younger adults, shifting the burden of disease. For example, incidence rates in women 50-64 years have surpassed those in men, and rates in women under 50 are now 82% higher than their male counterparts, up from 51% in 2002. This pattern includes lung cancer, which is now higher in women than in men among people younger than 65 years old.”

Rebecca Siegel
Rebecca Siegel, senior scientific director, surveillance research at the American Cancer Society and lead author of the report, said, “… progress is tempered by rising incidence in young and middle-aged women, who are often the family caregivers, and a shifting cancer burden from men to women, harkening back to the early 1900s when cancer was more common in women.”
Then, there’s a gender gap in funding research in the U.S. The ACS doesn’t talk about this.
Government and private funding in the U.S. for breast cancer research far exceeds that for prostate cancer. Some would put it this way: gender inequity
Some background
In 1990, women with breast cancer were rising up angry.
Women with breast cancer really spoke out loud and clear for change at the start at the ‘90s.
Led by the Dr. Susan Love, a famed breast surgeon, BrCa activists took a leaf from AIDS activists who in the 1980s changed the world of medical research by advocating for increased funding and increased patient involvement in research.
Remember back in the 1980s, when President Ronald Reagan ignored the AIDS epidemic. First Lady Nancy Reagan and Conservative U.S. Surgeon General C. Everett “Chick” Koop helped to steer the president to recognize the horror of the AIDS epidemic, which was decimating a generation of young gay men, and then, ultimately transformed the condition into one that could be lived with rather than a death sentence.
Protests paid off for groups like ACT-UP, the AIDS Coalition to Unleash Power. They also did for the women.
Dr. Love, who died from a blood cancer in 2023, noted in the Cancer History Project, that breast cancer activism “sort of evolved around the same time as the AIDS movement, because really, AIDS was the first time we had people with a disease lobbying and really involved in the research. And so, it was around that time, and that’s what really pushed us.”
As a Chicago Sun-Times medical reporter, I covered ACT-UP die-ins and a protest inside the annual meeting of the American Medical Association
Marching topless
After the publication of the first edition of her best-selling “The Breast Book,” Love spoke to a group of “older” women in Salt Lake City. “She felt her speech was going on too long and was a bit ponderous, so to lighten things up, she suggested they all go to DC and march topless to the White House demanding attention to breast cancer. [She] waited for the laugh, but what she got was a resounding ‘Sign us up!’”
The activists melted the hearts of the male-dominated Congress, whose members wanted to help their moms, wives, sisters, daughters and constituents who were impacted by breast cancer.
New research funding was made available through a unique program with the Pentagon, which had a pretty bad PR hangover from the Vietnam War and saw that it might win over the civilian population by set loose its researchers to address breast cancer.
In 1992, Congress funded the Department of Defense's (DOD) Congressionally Directed Medical Research Programs (CDMRP). The CDMRP initially funded research on breast cancer and eventually added other diseases, including prostate cancer.
From fiscal 1992-2023, CDMRP has allocated $4.2 billion to breast cancer research and $150 million in fiscal 2024. In comparison, the program allocated $2.3 billion to prostate cancer in fiscal 1993-2023 and $110 million for fiscal 2024.
Notice the gender gap.
I served as a citizen reviewer of research for the DoD program. We were basically told to focus on studies aimed at helping men with advanced prostate cancer, though I recommended studies I thought could help men on Active Surveillance as well as others.
A top researcher, who long has been involved with this program, told me CDMRP in its early years included research on Active Surveillance, but no longer doesH, e told me he simply feels it’s wrong.
I asked CDMRP the about this. A spokeswoman for the program confirmed that the program focuses on lethal cancers.
She explained in an email when I asked:
“Q: Why is lethal prostate cancer emphasized over low- or intermediate-risk prostate cancer?
“A: According to the American Cancer Society, ~85% of prostate cancers are considered low/intermediate risk and are typically handled through a period of “active surveillance” without intervention of any kind, or in some cases with surgery and/or radiotherapy followed by active surveillance. This active surveillance period can last from months, to years, to a lifetime before further clinical action is taken.
“In these cases, the patient’s prostate cancer is rarely determined to be the cause of death. The PCRP Program Book outlines how PCRP emphasized the need to focus on this small, but highly significant subset of tumors, since they are ultimately responsible for patient mortality. Therefore, they require the highest priority for new understanding and intervention strategies. While treatment for lethal prostate cancer has been a significant area of focus for PCRP-supported research, PCRP also invests in other overarching challenges, such as quality of life and survivorship, health disparities, and the biology of the disease, including progression from low-risk to lethal disease.”
NCI and research
And let’s look at funding at the National Cancer Institute (NCI), the biggest government funder of cancer research in the U.S. NCI has been fgighting a long engagement against cancer. President Franklin D. Roosevelt signed he National Cancer Act in 1937. President Richad M. Nixon gave the NCI a boost in 1971 with the launch of the “War on Cancer.” Federal investment in cancer research from $500 million in 1972 to $7.2 billion in 2024.
In recent years, NCI has allocated $581 million funding for breast cancer research compared to $281 million for prostate cancer tesearch.
With the incomingTrump administration, Biden’s NCI and National Institutes of Health directors have resigned though no one knows what will happen to research funding.
The science community has been jittery as the Trump has said he will let proposed HHS Secretary Roberty F. Kennedy Jr. “go wild on” health, medicines, and food policy. Kennedy has called for new directions at thge Nationsal Insitutes of Health, of which NCI is a part, and an either -year “break” in NIH funding for infectious diseases and would instead move money to chronic diseases like cancer.
Circling back to ACS research bucks
On the private side of cancer research funding, American Cancer Society funding of prostate cancer has consistently lagged behind that for breast cancer. Just like NCI.
In 2024, ACS spent $121.1 million on breast cancer vs. $37 million on prostate cancer. It allocated $67 million for lung cancer research and $62 million on colorectal research.
ACS last year said it was stepping up its efforts to help Black men, who are hard hit by prostate cancer.
William Dahut, MD, PhD, chief scientific officer for the ACS, in an article I wrote for Medscape last year denied any gender bias in research funding. He said the group makes funding decisions "based on finding the most impactful science regardless of tumor type. Our mission includes funding every cancer, every day; thus, we generally do not go into our funding cycle with any set-asides for a particular cancer."
In any case, over at ACS, there clearly is a funding gap between breast and prostate cancer.
Consider this at if you’re contemplating making donations to cancer charities: Ask what the charity done for prostate cancer patients like you lately?
And likewise, talk to your members of Congress to boost funding of prostate cancer research. (Here is a paper I wrote for a grad school class on how to lobby on health issues.)
Global patterns in prostate cancer: PCa is No. 1 cancer in men in 2/3rds of countries
By Howard Wolinsky
Internationally, patterns in prostate cancer vary.
Incidence can vary from No. 1 most common cancer in men, while other countries rates are lower based on use of early detection, genetics and other factors.
Freddie Bray, PhD, section Head of the Cancer Surveillance Section at the International Agency for Research on Cancer (IARC), in Lyon, France, et al. reported in 2022: “In men, prostate cancer ranks as the most frequently diagnosed cancer in 118 countries, followed by lung cancer in 33 countries, with liver, colorectal, and stomach cancer ranking in first place in 11, nine, and eight countries, respectively.. In terms of cancer deaths, lung cancer leads in men in 89 countries followed by cancers of the prostate (52 countries) and liver (24 countries). In contrast, two cancer types dominate as the most commonly diagnosed cancers in women, namely, breast cancer (157 countries) and cervical cancer (25 of 28 remaining countries.”
Prostate cancer is the most frequently diagnosed cancer among men in almost two thirds (118 of 185) of the world’s countries. Incidence varies markedly by region, and rates range from 6.4 to 82.8 per 100,000, with the highest rates seen in Northern Europe, Australia/New Zealand, the Caribbean, and Northern America and the lowest rates seen in several Asian and African regions. The regional patterns of mortality rates do not follow those of incidence, with the highest mortality rates found in the Caribbean and sub-Saharan Africa, indicative of disparities in early detection and treatment.
Prostate cancer is the leading cause of cancer death among men in 52 countries, including many countries in the Caribbean and sub-Saharan Africa, in Central and South America (e.g., Ecuador, Chile, and Venezuela), as well as Sweden in Europe.
ASPI seeking nominations for its 2025 awards program
Active Surveillance Patients International (ASPI) is inviting the surveillance community to submit ideas for its fourth 2025 awards program.
The awards program includes the Chodak Award honoring the late Dr. Gerry Chodak, ASPI’s first medical advisor and a University of Chicago researcher who encouraged the development of early conservative approaches to prostate cancer.
Winners have included such pioneers as Dr. Laurence Klotz, of the University of Toronto, Dr.Peter Albertsen, of the University of Connecticut, and Dr. Peter Carroll, of the University of California, San Francisco. All were early advocates and researchers of the protocol now known as Active Surveillance.
(For videos on all awards presentations, go to: https://aspatients.org/awards/)
Two other awards are now presented:
--The ASPI Special Awards to groups or individuals who have made major contributions to AS research. Winners have included Drs. Freddie Hamdy and Jenny Donovan, who were the principal investigators of the landmark ProtecT trial, which proved the safety and effectiveness of AS, and the Michigan Urological Surgery Improvement Collaborative (MUSIC) for its success in demonstrating how AS can be widely accepted in small or large practices in the community or academic urology practices, alike.
--The ASPI Patient Advocacy Award is named for ASPI co-founder Thrainn Thorvaldsson, the first recipient, and E. Michael Scott, founder of Prostate Cancer International, an early advocate for AS even though he doesn’t have prostate cancer.
“If you have names of folks who have fought the headwinds, and showed courage in furthering AS, please send them to us with your justification,” said Mark Lichty, ASPI chairman and co-founder.
Send your nominations to contactus@aspatients.org by Jan. 31, 2025.
MRI-invisible lesions: A good sign—like a Gleason 6?
By Howard Wolinsky
Did you know that it’s possible for prostate cancer can be confirmed by a pathologist but the lesion can be invisible in an MRI?
Is this a good thing? Many researchers think it is.
Dr. Mark Emberton, Professor of interventional oncology at University College London and Dean of its Faculty of Medical Sciences, will be speaking to the ASPI webinar about MRI-invisible lesions on Saturday, January 25, 2025, from noon – 1:30 p.m. Eastern (5:00pm-6:30pm UK time). Emberton is a pioneer on the use of MRIs in diagnosing, classifying and monitoring prostate cancer.
Don’t be invisible. Register here: https://zoom.us/meeting/register/tJYldu-qqzojGNEzCkgPQuTOWYGhcL80Dhec'
MRI-invisible lesions are considered a good thing comparable to Gleason 6.
Professor Emberton’s clinical research is aimed at improving the diagnostic and risk stratification tools and treatment strategies for prostate cancer (PCa). He specializes in the implementation of new imaging techniques, nanotechnologies, bio-engineering materials and non-invasive treatment approaches, such as high intensity focused ultrasound and photo-dynamic therapy.

His research has been published in over 300 peer-reviewed scientific papers in journals including BMJ, Lancet Oncology and European Urology. He has also contributed to the development of guidelines for the management of PCa and lower urinary tract symptoms, published by the International Society of Geriatric Oncology and the European Association of Urology.
If you have questions, please send them to: contactus@aspatients.org
You lead the way, Harley.
There was a men's march in 2018--suposedly federal f research funding doubled. But it was a lame affair compared to what the women with breast cancer and the AIDS patients did.
Sure, give women priority .. but how much priority? The gender gap is huge.
Are there really that many mopre and better leads on breast cancer than prostate cancer.
Women have been smarter and more aggressive in lobbying for funding.
Howard
We men should come out swinging! Let's drop trou and march on DC!
Seriously, women are the bearers of our children, they must have priority.