

Lessons learned: Retired college prof's Active Surveillance journey

Note: Readers of The Active Surveillor have told me they like first-person stories about our experiences with lower-risk prostate cancer. So join retired Prof. Harley Myler on his AS journey. Let me know if you have a tale to share. Harley has a great one.—Howard Wolinsky)
By Harley Myler, PhD, PE
Let me start by saying that as of this writing I am 71 years old. When talking about Prostate Cancer (PCa), age is very significant because with age comes a number of confounders that can generate confusion and propagate misinformation.
A diagnosis of PCa for a cis-male man in his 40s or 50s is significantly different from one in his 60s or 70s. Many have heard the expression more men die with prostate cancer than because of it, and this speaks to this point because low-volume, low- to intermediate-risk PCa is practically a given by the time a man is 70.
Of course, there are a large number of 70-year-olds who don’t have a hint of anything going on at all with their prostates—and now we come to the stochastic aspect of pretty much everything in medicine. A 27% chance of this, a low likelihood of that, and on and on. The burden on the informed patient is to determine, as accurately as possible, where he is with respect to this probabilistic pool.
In 2008 (I was 55) my PSA was 2.8, then 1.5 (56), then 1.9 (57), then 1.8 (60), then 2.2 (63)—very normal and no cause for alarm, the alarm came the next year when I was 64 and it had jumped to 7.2. When that result was seen by my internist he went into panic mode (anything above 4.0 is concerning). He immediately put me on antibiotics and referred me to a urologist (Uro).
By the time I got to the Uro my PSA had dropped to 3.9, but he wanted to do a biopsy anyway. I said no, and that was the first encounter I had with the ‘‘biopsy happy’ Uro, because the PSA jump was obviously due to prostatitis. I am guessing he was putting his kid through college at the time because they make next to nothing by doing a Digital Rectal Exam (DRE) and that in itself proved quite interesting to this story.
He did not give me my first one. I had had a few from my internists over the years and they always seemed pointless and very, very fast. I’m not complaining mind you, I just wondered how they could tell anything with such a short touch. In retrospect I think they wanted it over as quickly as I did.
The Uro, who gave me a DRE after my PSA jumped, commented that I had a very small prostate. I recall saying “Isn’t that good?” and him explaining that a small prostate producing a specific PSA reading is worse than a large one producing the same amount. That was my first introduction to the concept of PSA Density, an extremely important piece of data, which is the PSA reading divided by the gland volume. Obviously, you need an accurate volume, and you will not get that at all with a DRE.
(Sidebar on DRE: The DRE only allows the clinician access to the back part of the gland, yet some of them continue to use it to “estimate” volume, which is a colossal mistake. Volume of the gland is the second most important parameter when evaluating it for disease, the first being PSA. When I started my “journey” with PCa, the first Uro I saw after an elevated PSA declared that I had a “very small prostate” (based on DRE) and wanted to do a biopsy.
“I refused and my PSA dropped like a rock because my internist prescribed antibiotics anticipating prostatitis. Years later, after another jump, my new Uro estimated 30cc based on DRE. He updated it to 76cc after TRUS and then this year it was declared 83cc by the ‘gold standard’ MRI.
What this means is that at 30cc my PSAD was 0.21, very bad according to Dr. Jonathan Epstein, the renowned pathologist,. At 76cc it was 0.08 (very good) and at 83cc it was 0.065 and that helped me get a PI-RADS of 1. I mentioned this to my current Uro, who is monitoring my AS, and she said that Ultrasound was fine as it is close enough to the MRI volume and much cheaper and easier to obtain. Regardless, the first datum that should be obtained once one experiences a PSA blip is prostate volume. Research shows that PSA level is directly related to it.
My prostate settled down after that and in 2000 after retiring and moving hallway across the country, my PSA was a respectable 2.9 (I was 67), but a year later it was 4.2 and that set off the alarm again, so off to a new Uro. This new Uro was getting ready to retire, which he did the same month I elected to do AS, and as far as I was concerned it meant that he had seen it all.
My Uro did a DRE and concluded that my gland was a small, normal 30 cc. He also called for a PSA test, but the blood draw was after the DRE due to some confusion by the nurse. I already knew that a DRE makes a prostate more uncomfortable than its owner. My PSA came back 6.33 so once again ‘biopsy’ came up. I said no so he called for a SelectMDx report.
I want to state at this juncture that years ago I had asked why seminal fluid wasn’t checked for PCa biomarkers. Well, that is exactly what the SelectMDx test is all about.
For those of you unfamiliar with it, it starts with what the Uros call a “vigorous DRE,” and yes, it is as bad as it sounds. If you think a “normal” DRE is uncomfortable, you have no idea how bad a vigorous one is. Then you urinate into a vial that contains a fixative and the vial is sent off for analysis. After the DRE when I stood up to pee into the vial I exclaimed “It’s WHITE!” referring to what I saw at the tip of my member. My Uro said “Great! That’s what we want!”
The SelectMDx report comes back with two numbers, the likelihood of PCa detection at biopsy (mine was 74%) and the likelihood of detecting Gleason score ≥7 cancer (mine was 47%). This was when I finally realized what a crapshoot cancer detection, treatment and lifespan is. After the test, my Uro told me that we needed to do a biopsy and I remained adamant about not doing one. I asked about MRI, about fusion, etc., etc., because I was beginning to learn all the terms and techniques surrounding the issue. He finally convinced me to let him do an in-office Trans Rectal Ultra Sound (TRUS} biopsy which is the most unpopular, disliked, feared and hated procedure in Urology. Sorry, I may be exaggerating.

(Harley, out on a ruck—hiking with a weighted pack, a rucksack—at Carolina Beach State Park in October 2024.)
My main concern was that in order to ensure the safety of the procedure they blast you with antibiotics because the chance of sepsis from the biopsy needles piercing the rectum to get to the prostate is high. This wipes out your gut biome, and I was not happy about it. But I bit the bullet and received an antibiotic injection the morning of the procedure. Then, I went in and lost whatever dignity that I may have had. I will not go into the procedure here, but will say that the only pain I experienced was the initial numbing injections and I will take those any day over a visit to the dentist that involves Novocaine.
What I learned from the biopsy is that any procedure involving the prostate is very, very dependent on the skill and experience of the Uro. Mine had done TRUS so many times, it was a walk in the park for him and that skill translated over to the ease I experienced. From 12 samples, the standard pattern that is used on a “blind biopsy,” only one “core” was found to be malignant by the pathologist and it was graded Gleason 3+3=6. I will not go into the details of the Gleason scoring system and many Uros are abandoning it anyway for more clear and descriptive terminology, but this score meant that my cancer was not aggressive and most likely would not go any further. At this writing, there is a debate raging as to whether or not this grade should even be called cancer.
Nevertheless, I had a cancer diagnosis, and it was time to dig deeper and consider treatment options. If you are guessing that a possible treatment for such a low-grade, non-aggressive tumor is to do nothing (Watch and Wait) or keep monitoring on a schedule (Active Surveillance) you are getting ahead of me.
My Uro then instructed the pathologist to send the sample out for what is known as a Decipher test conducted by Veracyte Labs in San Diego. This test analyzes the DNA of the tumor itself, and the results are used to determine how extensive the treatment needs to be.
Thankfully, my Decipher score was 0.25 (Decipher produces a single value) and that meant “low risk,” very low in fact. On my Decipher report it stated that “Clinical studies have shown that Decipher low-risk patients have a favorable prognosis and these patients may be ideal candidates for Active Surveillance.”
When the results came in my Uro explained everything and then discussed treatment options. Radical Prostatectomy (RP), radiation, chemo, and Active Surveillance (AS). I have heard a number of men who felt that their Uros pushed aggressive treatments, but the simple fact is that they have to. If a Uro did not offer and explain ALL the options and a man went on AS and later died from PCa there might be litigation. When I told my Uro that I wanted to do AS, he seemed quite relieved.
During the biopsy my prostate volume was measured via the ultrasound equipment and as I explained earlier, accurate volume is very important with respect to PSA. Regardless of what you think about PSA, it is extremely valuable in guiding strategies. After DRE my Uro had estimated my gland volume to be 30cc and that means that with a PSA of 6.33 at biopsy, my PSA Density was 6.33/30 = 0.211.
This was not good as it indicated a small gland was producing a lot of PSA. The cutoff value for density is 0.15 (established by Jonathan Epstein, a famous uropathology researcher). However, during TRUS the size of my gland was calculated to be 76 cc, over twice the DRE estimate! This knocked my PSA Density down to 6.33/76 = 0.083, a nice low value.
During the TRUS I heard my Uro say under his breath, most likely when he saw the volume data, “Damn BPH.” He explained that the posterior lobe of my prostate, specifically the peripheral zone, was small and that is what is felt during DRE. The anterior and lateral lobes had BPH or Benign Prostatic Hyperplasia and accounted for the large volume of my gland. I won’t go into details, but this is a confounder condition for PCa because it is benign, but it causes PSA to rise because it causes the prostate to grow. It is age related and can cause urinary issues if the enlargement narrows the urethra.
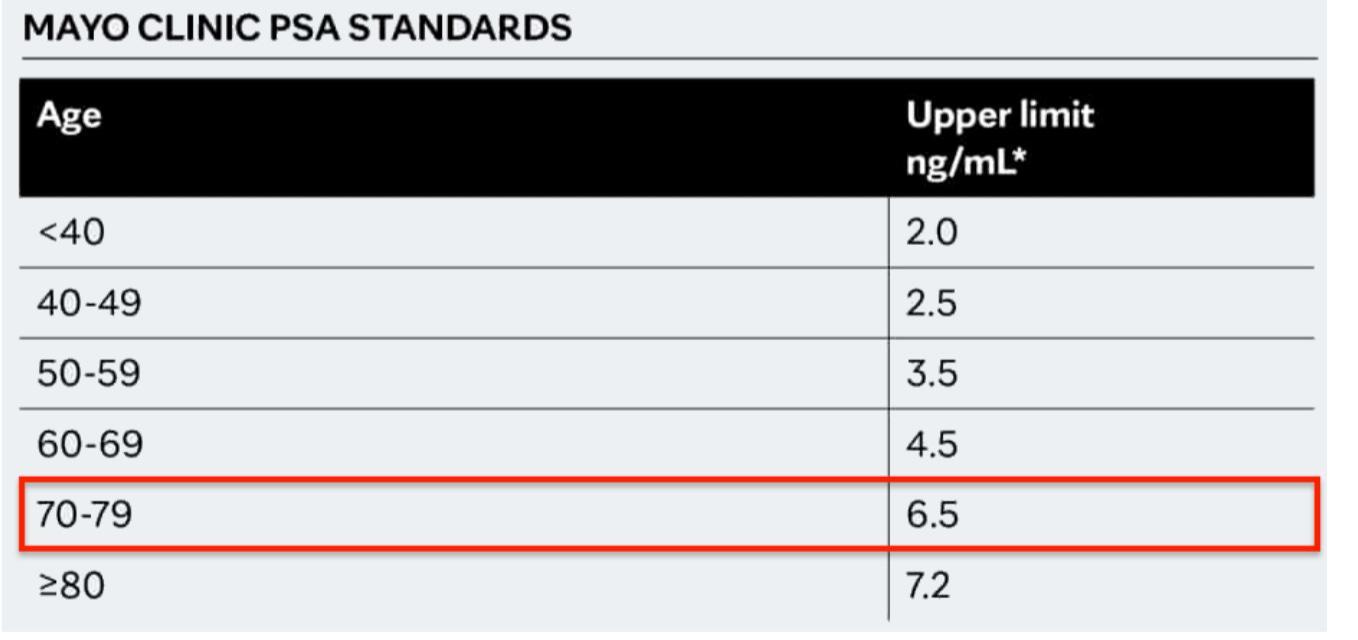
The Mayo Clinic published a chart that speaks to the BPH issue, and I have reproduced it below. There is a red box around the 70-79 group, which I am in, and the upper limit of 6.5 ng/mL is above my reading of 6.33 ng/mL—another ‘good to know’ data point.
After six months on AS, I went for my first checkup that consisted of a DRE, PSA and testosterone level. After I was diagnosed six months prior, my Uro told me that I would be referred to another Uro in the practice for my AS monitoring since he was retiring. He asked if I had any issue with a woman as some men don’t like the idea. I said no, that would be fine and then I told him that she had to have skinnier fingers than he did and I was right!
My PSA was 4.26 giving a density of 0.142 so my new Uro was happy and I went home. By the next AS visit in March 2024, my PSA was 5.48 and judged no issue by my Uro since it was still lower than my pre-biopsy level and consistent with that of a man my age.
The third and most recent visit was in October 2024 and it was Multiparametric MRI (MP-MRI) time. My PSA at that visit was 5.42, a slight drop, but AS protocols suggested an MP-MRI and I was anxious to get one anyway. My Uro ordered a 1.5T MP-MRI at a local radiology clinic. She had told me that if I wanted 3T I would need to go to Raleigh, N.C., but pointed out that the procedure done locally had produced good results in the past. Given the somewhat benign nature of my disease so far, I opted for convenience.
The MP-MRI report included a PI-RADS (Prostate Imaging Reporting and Data System) analysis where a radiologist analyzes the scan data and delivers a score, from 1-5, of the “Likelihood of clinically significant PCa” where 1 is Very Low, 2 is Low, 3 is Intermediate, 4 is High and 5 is Very high. My score was a 2, and I will say I was not surprised. The report from the radiologist was quite interesting as he confirmed “Benign-appearing hyperplastic stromal nodules,” which is BPH, but more importantly “No index lesion to suggest high-grade malignancy.” The report also stated that the capsule was intact and that is very significant as that is how aggressive lesions that are moving out of the gland can be identified. Once the capsule is breached no focal therapies are possible. His final statement was reassuring: NO INDEX LESION TO SUGGEST HIGH-GRADE PROSTATE MALIGNANCY. (In caps because that was the way it was in the report.)
So here I am, hardly cancer free, but certainly not too worried. I will stay on AS however, because PCa can take sudden and dangerous turns. Since my diagnosis I have worked fervently to become what I call ‘Hippie Healthy’ and it is ironic that I started this two years ago and only recently a number of major studies have identified the significance of diet and exercise to PCa treatment outcomes. I am one of those who consider AS a “treatment,” but that really is just semantics.
To get Hippie Healthy you start with a plant-based diet, and that does not mean vegan or vegetarian diet although those are more than adequate. I am a fan of the Mediterranean Diet myself. Add exercise, preferably HIIT (high-intensity interval training) and weightlifting. Get good sleep—deep, restorative sleep. Lastly, practice mindfulness. This does not mean religion although religion is fine. Options include meditation, yoga, Tai-Chi, etc. anything that will get you in touch with the cosmos. The goal is stress reduction because a prostate gland hates stress. Also keep in mind that fat reduction, if you are overweight, is necessary as well—have you ever seen an overweight hippie?
The following sums up what I learned:
· A man’s age is very important in establishing the probabilistic clade that he is in with respect to PCa.
· The experience of your medical team is just as important as their knowledge. Ideally, you want senior clinicians (experience) and young ones (fresh knowledge).
· If you do not join your team you will be confused and stressed. The more eyes and opinions on the issue the better.
· PSA remains an important tool in the complex arsenal of tests available, although it is subject to any number of confounders.
· BPH is a confounder and should be characterized before anything radical is proposed.
· Accurate gland volume is essential as analysis moves from detection towards treatment. DRE volume determination is useless, but modern ultra-sound volumes are comparable to those from MRI (the gold standard).
· General health changes the game. Get lean (diet), get mean (exercise), get unconscious (sleep) and get mellow (mindfulness)—Hippie Healthy.
Good luck with your journey!
Bio: Harley Myler currently resides in Wilmington, N.C., where he retired in 2020 after over 40 years in higher education. He currently remains on the faculty at Lamar University in Beaumont, Texas, as an Emeritus Professor and the Mitchell Endowed Chair in Telecommunications.
Prof. Myler has quipped that he didn’t quite retire because as an emeritus professor he remains, somewhat morbidly, on the faculty for life. The position includes his university email account and his webpage on the Department of Electrical & Computer Engineering website. Other pluses are that he doesn’t do any teaching, need not worry about publishing and attends no meetings. Regrettably, the downside is that he doesn’t get paid.
He is married to his very tolerant wife Nancy who also had a career in education as a Media Specialist (K-12 school librarian) and they have two children, Krifka (Director of Merchandise, Barnes and Noble Corporate) and Logan (Assistant Professor, University of Pittsburgh Medical School & Hillman Cancer Center) and two grandsons. When Logan was about four years old, and keep in mind that he was quite precocious, someone asked him “Where does your Dad work?” and he answered simply “He doesn’t work.” Hearing this I was somewhat shocked, but then he continued, “He goes to school; we all go to school. Dad goes to the university, Mom goes to the middle school, Sister goes to HS and I go to elementary.” In his mind, we were all just students and didn’t actually work. Now that’s an academic family.
Don’t miss this webinar: Is favorable intermediate-risk PCa the future of Active Surveillance?
By Howard Wolinsky
Kevin Ginsburg, MD, urologic oncologist at the Karmanos Cancer Institute/Wayne State University in Detroit, will be presenting a webinar for Active Surveillance Patients International (ASPI) entitled “Is favorable intermediate-risk PCa the future of AS?"
The program will be held from —12-1:30 pm Eastern, Saturday, Feb. 22. Celebrate President George Washington’s birthday with ASPI.
To register, go to: https://aspatients.org/event/is-favorable-intermediate-risk-pca-the-future-of-as/
Ginsburg is J. Edson Pontes, M.D., Distinguished Endowed Chair in Men's Health at Wayne State and co-director of the MUSIC prostate program.

(Dr. Kevin Ginsburg, co-director of the very successful MUSIC program in Michigan.)
MUSIC (Michigan Urological Surgery Improvement Collaborative) has been one of the most successful U.S. programs for Active Surveillance. Over 90% of patients with low-risk prostate cancer in its program go on AS vs. 60% nationally. Likewise, MUSIC has been successful in offering AS to patients with favorable intermediate-risk prostate cancer at a rate of about 45% compared with 20% nationally.
In 2023, ASPI presented MUSIC with its first ASPI AS ADVOCACY AWARD for its advances in researching and promoting Active Surveillance for lower-risk patients in place of aggressive treatments.
Check out my new Substack newsletter Prostate Cores, abstracts on research on PCa, biopsies, BPH, prostatitis.
Thanks, Harley's piece was outstanding.
Thanks fellow Fightin' Illini. I have two degrees from UI Urbana-Champaign. Also, I was a journalist-in-residence at UMich (Go Blue!) and am on faculty of Northwestern (Go Wildcats). I also lectured once a year at Harvard (Go Harvard Crimson!) on buisness ethics and medicine. I am working on an MPH now at UofI at Chicago,
Howard
As I read Harley's article about his experience of being diagnosed with low-grade prostate cancer, I thought, "This guy is a great writer and should teach men about prostate cancer." Then I got to the bottom of the article, where it says he is a college professor. That explains it!