
Stirring the Gleason 6 Pot--to Drop the Cancer Label
Stirring the Gleason 6 Pot--to Drop the Cancer Label

By Howard Wolinsky
Last week, Dr. Scott Eggener, vice chair of urology at the University of Chicago, and five other authors, including TheActiveSurveillor.com, shook up the prostate cancer world with doctors and patients alike choosing sides.
We proposed in an article in the Journal of Clinical Oncology that Gleason 6 no longer be called cancer.
Why? Because patients with Gleason 6, like most readers here, will not see the lesion spread and because the C-word triggers unnecessary anxiety and other emotional issues in patients like us that can drive us to unnecessary surgery and radiation. And finally, some of us experience financial toxicity, such as steep hikes in insurance rates or simply cancellation of our policies.
There was a big splash in the media with the paper. Our message reached millions and millions of patients with Gleason 6, which impacted many of our lives in unnecessary and unfortunate ways.
Here’s a brief and balanced overview on Channel 5/NBC News in Chicago: https://www.nbcchicago.com/top-videos-home/doctors-suggest-new-names-for-low-grade-prostate-cancer/2812015/
The managing editor of the Journal of Clinical Oncology, a prominent journal, said, “I’m pleased to inform you that your article, ‘Low-Grade Prostate Cancer: Time to Stop Calling It Cancer, was the most talked-about JCO article last week with 235 mentions on Twitter and a total Altmetric score of 1716 (combining social media attention, news coverage, etc.). This is already our second highest Altmetric score of all time. Congratulations!”
Good news on the Altmetric, whatever that is.
(The journal article can be accessed here: https://ascopubs.org/doi/full/10.1200/JCO.22.00123)
I know the vast majority of pathologists favor sticking with the status quo. They say said, “Gleason 6 looks like cancer.” That’s good enough for them.
I suspect that urologists have split down the middle on the issue as “Gleason 6 doesn’t act like cancer.”
Eggener, my former urologist, told me back in 2011 that he wanted someday to campaign to change the Gleason designation to a non-cancer. He told me recently that now was a good time for change because the evidence has piled up to drop the cancer label.
He helped me unsuccessfully fight a coverage cut in my term insurance policy,
Almost a year ago, Eggener and Ming Zhou, Pathologist-in-chief at Tufts Medical Center in Boston, debated the question at an AnCan Virtual Support Meeting for AS.
Zhou believed that if it looks like cancer, which Gleason does under the microscope, then it’s cancer. One of Eggener’s key points, in response, is that he has never seen a patient die from Gleason 6, so why call it cancer.
The question-and-answer period covered such issues as whether a high-volume Gleason 6 is riskier than a low-volume Gleason 3+4=7. Eggener argued that these Gleason 6’s could be risky. He also said not enough men with 3+4 go on AS.
The doctors engaged in an informative and entertaining cross-fire discussion that should not be missed.
So who won? Our poll showed that before the debate: 55% of respondents thought Gleason 6 was cancer, while 10% thought it wasn’t cancer. 35% were unsure.
The numbers changed dramatically after the debate: Only 22% thought Gleason 6 is cancer, 47% said Gleason 6 is not cancer, and 31% were unsure.
Eggener won the debate.
Then, something amazing happened.
The following day, Zhou got back to me saying he switched teams:
“Dr. Eggener has won me over. I am now in his camp. I just proposed to work together to educate pathologists on this topic. As you know, I am also the president of Genitourinary Pathology Society (GUPS, an international GU pathology society). I will do my part to change the name.”
He confirmed last week that he is sticking by Eggener.
I have been running a survey on what patients think now. You know what? So far, the proportion of patients who favor dropping the cancer label is still the majority:
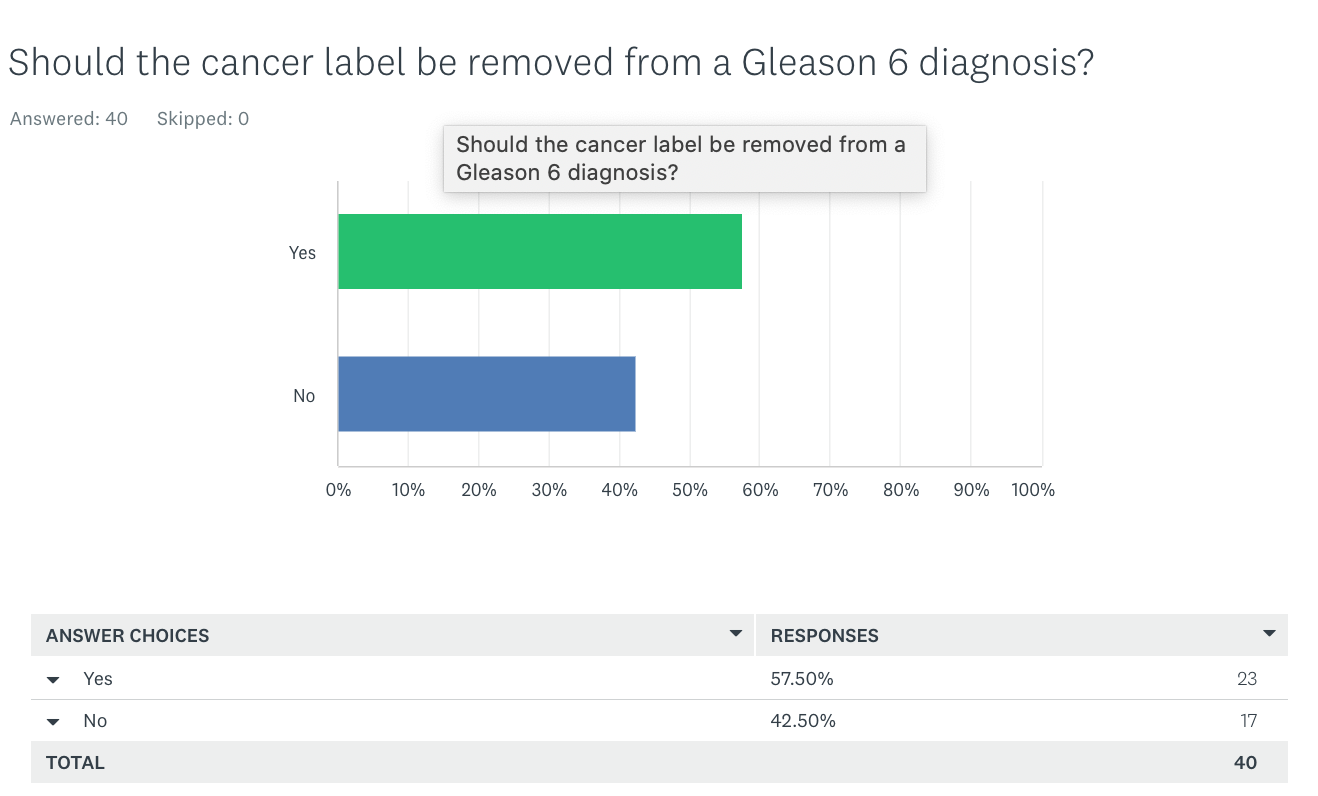
A minority say the diagnosis affected their insurance coverage.
So come on and vote: “Should the cancer label be removed from Gleason 6?”: https://www.surveymonkey.com/r/ZQHDQYK.
I will be running more commentary on both sides of the question.
How about signing up for a webinar on how lifestyle can affect prostate cancer:
AnCan is presenting a program on lifestyle choices and all grades of prostate cancer at 8-9:30 p.m. Eastern on May 31. Register at: https://bit.ly/3KkxcfC
The webinar, entitled “Optimizing Sleep, Exercise, and Nutrition in Prostate Cancer," features Dr. Stacy Loeb, professor of Urology and Population Health at the New York University School of Medicine and the Manhattan Veterans Affairs Medical Center, and Dr. Justin Gregg, assistant professor of Urology and Health Disparities Research at UT MD Anderson Cancer Center, of UT MD Anderson Cancer Center in Houston.
Did you miss the most prominent program on AS to date: “Your Voice in the future of Active Surveillance,” on April 22.? Here’s the link: https://aspatients.org/meeting-videos/
A Who’s Who of experts joined the conversation along with patients and advocates, who were not too shabby either.
Subscription rate to low even for those unable to absorb voluminous amount of.......................names, forget the research! Remember the stars next to your name in second grade as entering classroom, you know, next to the coat rack; gonna restart such for you now? Were I to wager, the battle you, ANCAN, ASPI started is not picking the right convert, doc and medical center alike, it's relentlessly beating into men importance of, "the art of the interview", ever so clearly shared with us all openly for "free." If we know what we should ask up front and elicit an uninformed response, "About face!" Do a multiple regression analysis of AUA member leaning over the years and bet response-2nd highest-no shock to anyone; follow the money!
What will you get for your pros mitzvah?