'Threading the Clinical Needle' on Gleason 6/GG1: A Matter of Language and Math

By Howard Wolinsky, Editor, The Active Surveillor
For years, the fight to remove the “cancer” label from “pure” Gleason 6 prostate cancer, which doesn’t spread and doesn’t kill, has been a high-stakes balancing act. Now, leading experts believe they have finally found the exact words to “thread the needle,” meaning successfully navigating a very delicate, difficult, or complex situation that requires extreme precision and leaves no room for error.
Pure Gleason 6 (Grade Group 1) is so indolent it essentially lacks the capacity to spread or kill, yet the terrifying “C-word” routinely drives men into unnecessary, life-altering surgeries that can result in erectile dysfunction and incontinence.
I have campaigned for years alongside AS thought leaders, including UCLA’s Dr. Scott Eggener (my former urologist at UChicago), Memorial Sloan Kettering biostatistician Andrew Vickers, and UCSF urologist Dr. Matthew Cooperberg, to relabel it as a noncancer.
The goal with the name change is to reduce patient anxiety and to reduce “financial toxicity,” such as insurance and job discrimination.
But bringing the rest of the medical establishment—and many patients, for that matter—on board required striking a delicate linguistic compromise that acknowledged the genuine fears of both cautious doctors and anxious patients.
A Thought Experiment That Could Save Lives
The turning point in this debate is a new modeling study published in JAMA Oncology, last week by lead author Vickers and senior author Eggener. along with Cooperberg and Peter Carroll, chair at UCSF, and Christian Pavlovich, head of the AS program at Johns Hopkins.
All are recognized leaders in AS. Carroll was one of the pioneers who introduced AS in the 1990s, but he also up to now, resisted redefining Gleason 6.
The study crunches the numbers on what would happen if we stopped calling Grade Group 1, or Gleason 6, a cancer and instead labeled it a “precancerous” condition.
Cooperberg told me he was thrilled to finally see this data published. “It’s kind of nice to see this out because we’ve been talking about this concept with multiple modeling groups over the years,” he explained. “Andrew (Vickers) ran this model... and there is some sensitivity analysis in the paper. An X range of additional deaths from prostate cancer in the AS cohort balanced against an X increase in screening. It’s a thought experiment, but it’s a really valuable and important one.”
The math overwhelmingly favors the change. By dropping the cancer label, the sheer terror that keeps the general public away from PSA screening evaporates. “The flip side is, if you change nomenclature, the balance of harms and ratios of PSA screening goes way down,” Cooperberg said. “The rationale for screening becomes almost unassailable.”
Otis Brawley’s Endorsement
When a major paper like this drops, the accompanying editorials can make or break its reception. In this case, the editorial was penned by Dr. Otis Brawley, the Johns Hopkins public health titan and former chief medical officer of the American Cancer Society. Epidemiologist Brawley has been notoriously critical of prostate cancer screening, frequently calling out the overtreatment pipeline.
During our interview, Cooperberg candidly admitted he was nervous about what Brawley might write. “There is an editorial by Otis Brawley that I’ve not read yet,” Cooperberg told me. “Partly because I am dreading it, but I actually don’t know what he said, whether it was favorable or not.”
Cooperberg didn’t need to worry. Brawley actually endorsed the nomenclature change. Brawley recognized the grand public health compromise at play. “By reducing risk of unnecessarily aggressive treatment, more men will agree to prostate screening, leading to the diagnosis of more men with aggressive disease and more prostate cancer deaths being averted,” he wrote.
The Mystery of Carroll’s Resistance
That broad, life-saving potential is finally winning over some of the most prominent historic skeptics of relabeling, including Dr. Peter Carroll. As the UCSF urology chair and an Active Surveillance pioneer, Carroll resisted a name change.
Carroll’s prior concern was not simply a matter of semantics. It was that removing the cancer label could cause some patients to skip Active Surveillance, imaging, or repeat biopsies, even though a low-grade diagnosis can still be associated with undersampling or later upgrading.
He told me: “Renaming did not get widespread support and would be confusing (Does the human language need more clunky monikers?) to many. Precancerous implies no need to treat, follow appropriately. Perfect blend of risk (low) and reward (no side effects of unnecessary treatment). Also, we are getting closer to a modern, operational definition of cancer, not one disease but a spectrum necessitating a measured approach - like most human diseases - diabetes, cardiac disease, etc.”

Cooperberg said of Carroll: “He has always been pretty reserved about the idea of nomenclature change. I have had a lot of conversations with him. I’ve never been able to pin him down as to why. He just feels like it’s a distraction from just trying to do surveillance better. I never got a really clear answer on it, but he does seem to be evolving on this.”
Carroll told me his evolution crystallized around the specific phrasing proposed in the JAMA Oncology study. Instead of calling Gleason 6 “benign,” the study relies on the term “precancerous.” That choice proved to be the turning point for Carroll. In an email, Carroll explained why this won him over: “The BIG difference is the term precancerous, this threads the needle nicely.”
Cooperberg noted that the specific term “precancer” is what “is resonating with him [Carroll] specifically,” but Cooperberg himself isn’t rigidly tied to one specific label.
Epstein, the ‘Nay Camp,’ and Real Risks of Removing Cancer Label
Yet this linguistic debate gets at the heart of why relabeling is so fiercely contested. There is a vocal group of doctors and patients in the “nay camp” who strongly oppose dropping the cancer label. Prominent pathologists, most notably Dr. Jonathan Epstein, one of the top uropathologists in the world and former head at Hopkins, have spearheaded the medical opposition. Epstein has argued that if the “carcinoma” label is removed, men will drop their guard, skip their follow-up biopsies, and miss the window for a life-saving cure if their disease progresses.
This pushback isn’t just coming from doctors; it comes from patients, too. Whenever I suggest relabeling Gleason 6, I hear from a few men on Active Surveillance who worry that their peers will stop monitoring. Some men with advanced cancer that developed after they had been on AS or whose tumors were undergraded also object.
Cooperberg acknowledged that the medical risks of this change are real.
“There is definitely a class of folks out there that are in the nay camp on this, worried that we would not do surveillance and we would really lose track of people,” he said. “There’s all this concern about whether we will miss people and men will die because they didn’t take [surveillance] seriously... That number, by definition, is greater than zero.”
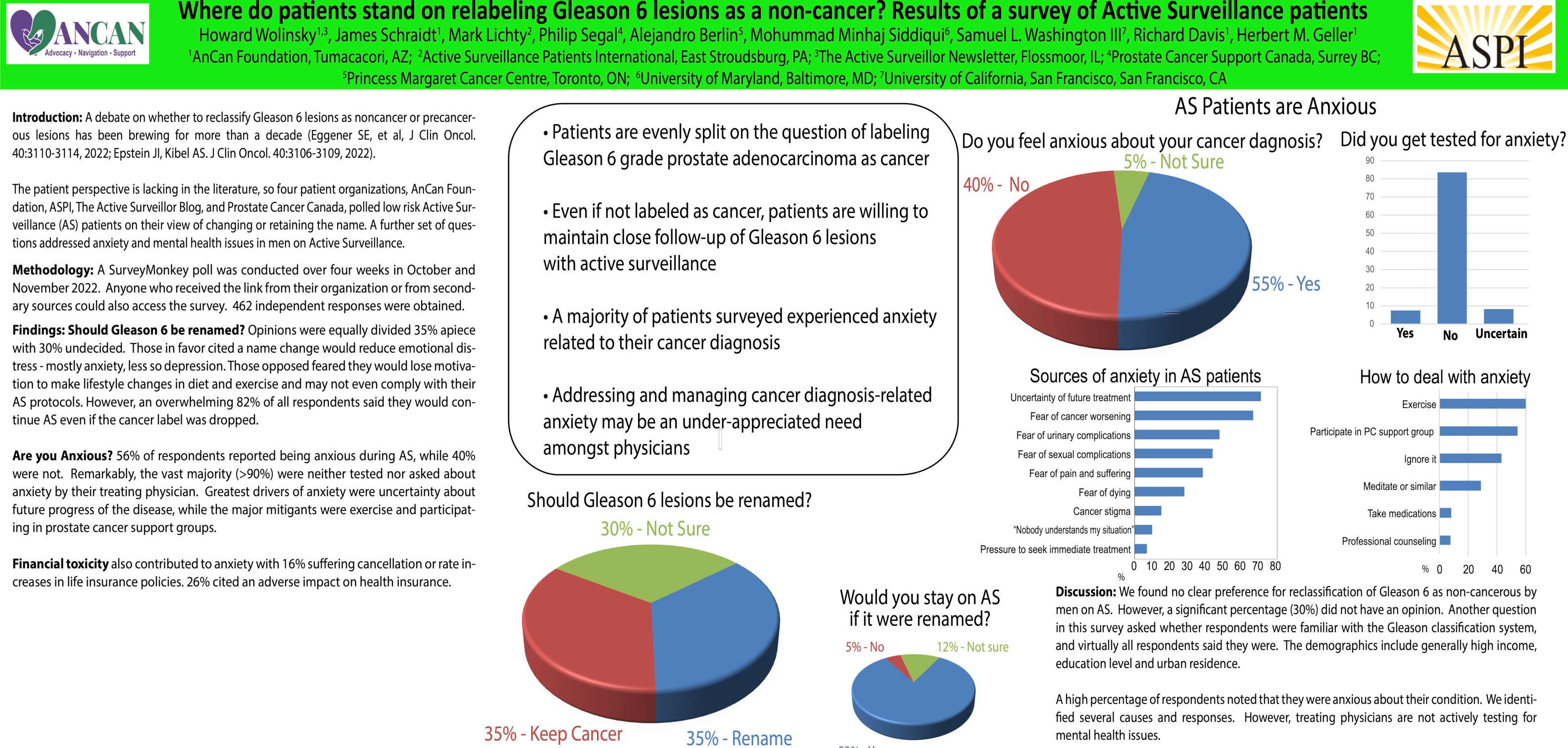
But then, there are other real-world data suggesting the fear that men will abandon surveillance en masse may be vastly overblown. A joint survey in 2023 by AnCan, Active Surveillance Patients International (ASPI) and Canadian colleagues of more than 450 patients on Active Surveillance found that if the cancer label were removed, only 5% of patients said they would quit surveillance.
Here’s the poster presented at the American Society of Clinical Oncology:
My four-minute talk—Yes, I can keep it short upon demand.— During an off-campus meeting, a $1 million allocation by the Centers for Disease Control was secured, which considered PCa a public health problem, for a study on patient views on, among other things, renaming Gleason 6. I thought $1 million was chump change, but this turns out to be one of the largest AS studies funded in the U.S.—the heavy lifting on AS was done in Europe. Cooperberg is co-principal investigator of the CDC study, along with Stacy Loeb, MD, of NYU. I am the patient advisor.
Gaining Momentum
Carrol, an opinion leader, represents an important defection to the yea camp.
Ultimately, leaders like Cooperberg and Carroll are realizing that you don’t have to choose between reducing panic and maintaining vigilance. Cooperberg said that with a change in the label “we would still follow men basically the same way.”
By "threading the needle," the movement to relabel Gleason 6 potentially is moving from a radical idea to mainstream consensus. The population-based math is simply too powerful to ignore. As Cooperberg concluded: “On balance, you save thousands, potentially tens of thousands of lives depending on what the assumptions are in the model.”
Check Out ‘This Guy’s Guide: The No-BS Health Report for Men 50+’
By Howard Wolinsky
I appreciate your subscription to The Active Surveillor. But there’s more to men’s health than the finicky prostate and its myriad issues.
In time for June’s Men’s Health Month and Father’s Day, I’m launching “This Guy’s Guide: The No-BS Health Report for Men 50+.”
In This Guy’s Guide, I will cover the full gamut of topics that concern us men over 50: wellness, exercise, diet, sleep, hypertension, BPH, heart disease, cancer, etc. Let me know what you think I should cover: howard.wolinsky@gmail.com
I aim to bring you the facts, often with a lighter touch, once a month.
Get a preview here: https://thisguysguide.substack.com/publish/post/196160545
I hope you will sign up for a free subscription, try it, and upgrade to a paid subscription if you’d like to support my work.
No pressure. No BS, either.

Biomarkers are starting to pull their weight in helping men avoid unnecessary biopsies.
At June’s ASPI webinar, we’ll be hearing from Dr. Jeffery Tosoian, a urology researcher from Vanderbilt, who has been much in the news lately because he helped develop the first biomarker validated for men on Active Surveillance, MyProstateScore2-AS. Also, Dr. Eric Klein, urology chair emeritus at Cleveland Clinic, speaks about another promising biomarker, IsoPSA,
The meeting is set for Saturday, June 27, from noon to 1:30 p.m.
Go to this link https://aspatients.org/event/a-new-era-in-prostate-cancer-testing/, scroll down and click the register button to get a front-row seat.