

Will renaming Gleason 6 as a noncancer help?
Top gun Jonathan Epstein, MD, of Johns Hopkins, weighs in with a resounding "No"

By Howard Wolinsky
When Jonathan Epstein, MD, speaks everyone involved with prostate cancer listens.
Dr. Epstein is director of Surgical Pathology at The Johns Hopkins Hospital. He is recognized as a leader in the field of urological pathology. He reviews the slides of well over 12,000 patients a year.
His views carry enormous weight for us as individual patients as well as in setting the policies that impact the field.
Bottom line. Epstein opposes renaming Gleason 6—AKA Gleason Grade Group 1.
(Epstein in 2013 introduced the use of the GG 1 terminology so those of us with Gleason 6 didn’t think we were at death’s door. Gleason 6 is the bottom score we could get. GG 1 helped reduce the fear factor. Thanks, Dr. E.)
Back in 2010, he rendered a second opinion on my biopsy. Ultimately, I was diagnosed with a less-than one-millimeter speck of Gleason 6, or GGG 1, “cancer” in a single core.

(Jonathan Epstein, MD)
One urologist said he could “cure” me if I underwent a prostatectomy in his OR the following week. He didn’t support Active Surveillance (AS)--careful monitoring of my lesion. I dumped him.
Not many urologists supported AS in 2010. Only 6% of patients took a leap of science (and faith) based on research by Laurence Klotz, MD, and a few others showing that surgery and radiation were not the only paths. Gleason 6 “cancer” was slow growing and the kind of “cancer” patients like me could live with and not die from.
Active surveillance offered a way to use PSA testing, MRIs, urology exams, and biopsies to follow the “cancer” and to intervene with time to spare if more aggressive cancer reared its ugly head.
Note the quotations around “cancer.” Even in 2010, some doctors didn’t think Gleason 6 should be considered a malignancy.
The day after my Gleason 6 was diagnosed, I saw Scott Eggener, MD, at the University of Chicago. He told me he didn’t think I needed surgery. He declared me the “poster child for Active Surveillance” and shared Klotz’s research with me. He predicted in 10 years’ time my so-called cancer wouldn’t grow.
Hard to believe that I came thisclose to getting unnecessary surgery and its potential side effects, including impotence and incontinence.
Eggener was right, even as I head into my pros mitzvah in 2023, 13 years on AS. In four subsequent blind (“pin the tail on the donkey”) biopsies, no cancer was seen again.
My new urologist, Brian Helfand, MD, PhD, of NorthShore University HealthSystem, told me that I may be done with biopsies and we can follow my so-called cancer with a type of PSA test (PHI—Prostate Health Index) and do an MRI should my PHI increase. (It actually—inexplicably—decreased 25% over last year.)

(Scott Eggener, MD)
Eggener invited several top docs, including Matthew Cooperberg, MD, Andrew Vickers, PhD, and Alejandro Berlin, MD, to write a think piece for the Journal of Clinical Oncology: “Low-Grade Prostate Cancer: Time to Stop Calling It Cancer.”
The basic argument boiled down to this: Gleason 6 looks like a cancer to a pathologist. But it doesn’t act like one. Many top urologists say it won’t kill you. So why call it cancer?
Gleason 5 and below have been undefined as cancer. Why not 6?
I was a co-author of the paper, providing a patient point of view. My main contribution was talking about the “financial toxicity” aspect, how my life insurance company wanted to cancel my policy after I was diagnosed and how seven other insurers refused to cover me because I had “cancer” albeit one that would not affect my life expectancy.
Eventually, my insurer (Transamerica) gave me a new policy for $100,000 for $200 per month, My old policy was $500,000 for the same premium.
(I wrote about this issue in TheActiveSurveillor.com in a piece entitled “Lies, dirty lies, and insurance discrimination.”)
As co-founder of support and advocacy groups for patients on AS, I have seen how the cancer diagnosis can result in anxious surveillance affecting about 33% of AS patients. The anxiety can be enough to push some to undergo unnecessary treatment and risk its side effects.
Eggener et al said: “Reclassification of GS6 would immediately lead to markedly fewer diagnoses of PCa; fewer men receiving radiation, surgery, and other treatments; fewer men experiencing treatment-related side effects; lower patient and family anxiety; and substantial reductions in financial burden to individuals and the health care system. No matter how much time a physician may spend downplaying the significance of a GS6 diagnosis or emphasizing the phrase low-risk, the words “you have cancer” have a potent psychological effect on most men and their families.”
(Journal of Clinical Oncology)
I had written about this in my blog at MedPageToday in January 2021, “Is This Really Cancer? — Movement builds to classify Gleason 6 prostate lesions as nonmalignant”
I wrote more on the issue in TheActiveSurveillor when the JCO paper came out.
I contacted Dr. Epstein for comment. But he said he couldn’t comment because he had been invited to respond to the paper by Eggener et al in April.
Epstein alerted me this morning that he and Adam Kibel, MD, chief of urology at Dana Farber in Boston, had responded in the Journal of Clinical Oncology to the Eggener paper.
Epstein is one of you--a subscriber to TheActiveSurveillor. He wrote me: “I know you have the opposite view, but as an objective reporter I hope you can share this with your readers for the counterview. Thanks. Jonathan.”
I’ll summarize Epstein’s arguments. But I urge you to read both articles and come to your own conclusions.
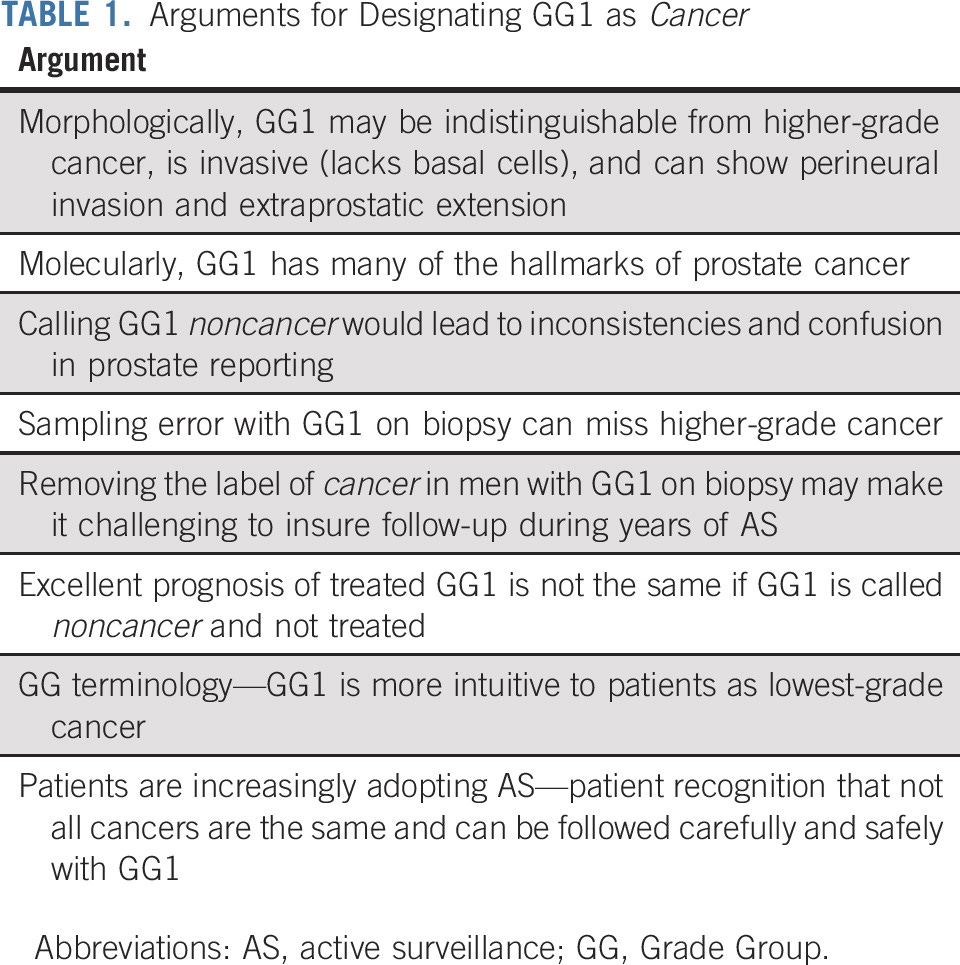
Epstein said: “Some of the most powerful reasons for not renaming GG1 prostate cancer with a noncancer diagnosis are related to practical patient care issues. First, a significant percent of patients with GG1 have grade reclassification necessitating treatment. Even in very low-risk disease, close to 15% will have higher grade on subsequent biopsy. The result is that follow-up for whatever noncancerous substitute terminology would be similar to current AS for GG1 cancer and a change to a noncancer designation would likely result in no change in management. Second, the grade of the tumor as GG1 is not the sole factor that should be taken into account in deciding whether to rename it as noncancer.
“Traditional factors, such as tumor volume and clinical stage, are also used to determine if a patient can safely be placed in AS. Increasingly, there are other factors that come to bear on management decisions such as genomics, genetics, and imaging. Would a patient with GG1 and a BRCA2 mutation be considered noncancer? Although mutations are rare, they do occur in men with GG1 and are associated with aggressive disease. Genomic testing, such as Decipher, Oncotype DX, and Polaris, has been added to our clinical armamentarium to further delineate the aggressiveness of the cancer.
“ Underlying all these tests is the concept that (1) patients can be risk-stratified using more than just Gleason Score and (2) patients at low risk still need to be monitored to ensure no clinical progression. Finally, multiparametric magnetic resonance imaging (mpMRI) increasingly plays a role in our management of men with indolent prostate cancer. PI-RADS 4 and PI-RADS 5 are associated with upgrading and therefore have been integrated into routine management. Should a patient with a PI-RADS 5 GG1 tumor on biopsy be told that they do not have cancer?”
Epstein worries that reclassification could cause confusion in reporting biopsy results to patients and their urologists.
He said: “From a practical viewpoint, how would needle biopsies be signed out where one part was GG1 and another part was GG2? Would the GG1 in this setting be called noncancer, confusing patients that they had two separate tumors? What is the scientific rationale that Gleason pattern 3 in GG2-3 … is cancer, yet Gleason pattern 3 in GG1 is not cancer although they are indistinguishable morphologically?”
Epstein also picked up on the argument that if Gleason 6 were reclassified as a noncancer, patients would not diligently follow the testing for AS, including MRIs and biopsies. (My current urologist is in that camp.)
Epstein said: “Removing the label of cancer in men with GG1 cancer on biopsy could make it challenging to ensure that they are carefully followed and biopsied sequentially during years of follow-up on AS. Eggener et al recommend that patients with GG1 should not be told that they have cancer, yet will still be expected to undergo close long-term follow-up with periodic repeat biopsies and imaging. Although patients with optimal insurance will likely not be affected by a change in terminology, those with policies that are less robust may fall into a trap where follow-up is curtailed when GG1 is renamed noncancer, and there is an increase in out-of-pocket expense. This is particularly an issue in underserved communities. Currently, patients already fail to follow up for AS. … close to 40% of all men and 60% of Black men with low-risk prostate cancer failed to follow surveillance strategies. It is logical and expected that renaming GG1 as not cancer will lead to less compliance with follow-up.”
(Journal of Clinical Oncology)
Thanks to Drs. Epstein and Eggener for debating this issue that is important for the patients diagnosed with low-risk Gleason 6 prostate “cancer.”
There is a solution to this naming game that has so far eluded science. Doctors agree that some of us have lesions that will never be a threat to us.
As Epstein notes--and I am sure Eggner would agree--”The underlying clinical conundrum is how to identify those patients and how that would alter management.”
The debate is a healthy thing. As you might suspect, a minority—maybe only 20%—of pathologists support dropping the cancer label from Gleason 6. About 50% of urologists support the change.
What should we do in the meantime?
Sound off in the comment bubble.
Also, please share your opinion in the comments and answer the survey: “Should the cancer label be removed from Gleason 6?”:
https://www.surveymonkey.com/r/85WMY77
Don’t miss the ASPI webinar, “Eat to Beat Prostate Disease,” on July 30 at 12-1:30 PM Eastern, featuring William Li, MD.
Free Registration: www.aspatients.org or go direct to: https://bit.ly/3t5lFLx
Free prostate-healthy recipes for all registrants.

Join Dr. Channing Paller, associate professor of Oncology and Urology at Johns Hopkins University, Sidney Kimmel Comprehensive Cancer Center, and Rob Finch, Director of Urology Medical Affairs at Myriad Genetics as they discuss the impact of genetic factors in prostate cancer and the PROMISE study.
Genetics, the PROMISE Study, and Prostate Cancer: a Town Hall Webinar
July 20, 6:00 p.m. - 7:00 p.m. Eastern Time
Meet the Speakers:
Dr. Channing Paller is associate professor of Oncology and Urology at Johns Hopkins University, Sidney Kimmel Comprehensive Cancer Center, and associate director for Oncology of the Johns Hopkins Clinical Research Network. She is a clinician scientist focused on translating basic scientific findings into treatments that will improve clinical outcomes and reduce toxicities for men with prostate cancer. Dr. Paller is a lead investigator of the PROMISE registry and, as an expert in clinical trial design, she leads multiple clinical trials of innovative new treatments and treatment combinations employing germline and somatic biomarkers. She earned her M.D. at Harvard Medical School and completed her medical residency and fellowship in Medical Oncology at Johns Hopkins.
-
Rob Finch is a Certified Genetic Counselor. He graduated with a Master’s Degree in Human Genetics from the University of Pittsburgh in May 2001. Rob worked at Memorial Sloan-Kettering Cancer Center from May 2001 to September 2003, where he led the Hereditary Colorectal Cancer Registry, as well as provided risk assessment and genetic testing to patients through the Clinical Genetics Service. In September 2003, Rob joined the Myriad Genetics Team, where he has served as a Regional Medical Specialist and Institutional Account Executive for the Oncology Division and currently serves as a Director of Urology Medical Affairs. Rob works to educate and provide clinical support to healthcare providers who treat prostate cancer for Myriad’s BRACAnalysis CDx®, MyRisk™ Hereditary Cancer Test, and Prolaris®.
Join a ZERO webinar, Prostate Cancer and the Unique Needs of the LGBTQIA+ Community featuring Anne Katz PhD, RN, FAAN, of CancerCare Manitoba, Winnipeg.
Register here:
https://us06web.zoom.us/webinar/register/WN_eUvLX0yNSAmRe5b-ST7zeg.
I looked in Google. They look very different. Prostatitis is a mystery in itself.
And another comment/question regarding renaming Gleason 6: What is the difference between Prostatitis cells and Gleason 6 cells?