A rural Kansas active surveillance patient shares his story as a medical migrant
Dr. Zhou's Pathology Report explains perineural invasion and active surveillance
By Howard Wolinsky
(Editor’s note: Life on the farm is probably nothing like I imagine. But I can picture my friend Richard Brensing driving his combine while listening to webinars on prostate cancer. Richard may live in the Kansas outback, but he is a well-educated low-risk (Gleason 6) prostate cancer patient thanks to attending webinars and often the AnCan Foundation Virtual Support Group for AS on most Wednesdays. This is third in a series on what I call the Dust Bowl of Urology, the lack of urologists andmodern prostate cancer care in rural areas, and how it forces men like Richard to be medical migrants, driving hours and hours and hundreds of miles to maintain active surveillance. Let me know should you want to share your story: mailto:pros8canswers@gmail.com—Howard Wolinsky.)
By Richard Brensing
Hello, my name is Richard Brensing. I am a farmer and live in Stafford, Kansas, a rural agriculture community of 900. We have a small rural hospital that includes services such as PT, OT, Lab, X-ray, swing beds, acute care beds, and an emergency room managed by a doctor offsite most of the time. There is no full-time doctor but do have doctors and PA’s who work rotations to cover the ER.
(Richard Brensing)
My prostate cancer story began in 2016 with my annual physical and my PSA being 6. My primary doctor, who was located in Hutchinson, Kansas, which is 45 miles away, scheduled an appointment with a urologist in that clinic. This happened to be the same urologist who diagnosed my father at age 70 with prostate cancer.
The urologist advised me to have a prostate biopsy, so that is what I did. He performed a 12-core transrectal biopsy with the results coming back negative. My PSA dropped over the next two years to 1.6. I continued to monitor my PSA every year.
In April of 2019, at the age of 63, my PSA had increased to 4.38 and my primary care doctor said I needed to see the urologist again. Learning that he had retired, I met with a new urologist who had taken his place. We discussed the increase in my PSA. He told me that I should have another biopsy. After more discussion, he suggested I could have a 4K test. I agreed and the test was performed.
The results showed that I would have a 9% chance of having an aggressive cancer. After more discussion with him and my wife, Shelly, we decided that the only way to know for sure was to have the biopsy. I traveled to his office in Salina, Kansas, which is 100 miles away, in June of 2019 for the procedure. He performed an 18-core transrectal biopsy, which was very uncomfortable. I am not sure why this experience was much worse than before but when I left the facility, I needed to be catheterized due to urinary retention. So, I headed back home with a catheter for three days.

(Richard and Shelly Brensing on their combine in Kansas as they finished the final wheat harvest before retirement.)
A week later, I met with the urologist in his satellite office in Great Bend, Kansas. The first thing out of his mouth as he entered the exam room was, “Well, you have cancer”. My wife and I were stunned, as we were expecting a good report.
The next question I asked was, “What would you do if you were in my shoes”? My urologist began to inform me of my options but said, “I would recommend a radical prostatectomy, but I am biased, of course, I am a surgeon”. He then began to share all of the side effects of a radical prostatectomy. He also quickly mentioned other options for treatment. The urologist stated that he could get me scheduled for surgery soon.
We then planned to meet in two weeks to discuss my decision. Shelly and I went home and began researching prostate cancer online and ordering books. I read a book on proton therapy and another book that contained information about many types of treatments that were available.
This information included active surveillance as an option. It was a very eye-opening experience that there were many other options available to me. I also understood that I needed to be an advocate in deciding what my prostate journey would look like.
I had my pathology report sent to me which showed less than 5% of prostate cancer in 1 of 18 cores, Gleason 3 + 3, so my diagnosis was low volume, low risk. When I met with the urologist at my follow-up appointment, I said that I was not ready to commit to any treatment especially not a radical prostatectomy, and that from what I have learned about low-risk prostate cancer, I was going to take more time to research so that I would be able to make a good decision for myself. I also shared that active surveillance was something I was seriously considering. He did agree that it was all right to take my time.
(Richard Brensing and (from left) grandsons, Parker, Emmett, and Cason.)
With more knowledge under my belt and support from my wife, and prayerful consideration, we both continued learning what we could about this disease. I feel that often we, in rural areas, agree with whatever our doctor directs us to do, not educating ourselves so that we can become our own best advocate.
I also began talking to some of my friends who were dealing with prostate cancer. One of them had been treated with Cyberknife near Denver. I contacted his doctor to discuss Cyberknife as a treatment. I also sent him my pathology report and after reviewing it, he suggested I consider active surveillance.
In my online research, I came across the Inspire community, where men ask questions regarding their particular PC diagnoses and receive very supportive replies. From this, I learned about ASPI, AnCan, UsTOO, now merged with ZERO, etc. groups focused on helping men with their prostate cancer journeys.
I have become involved with an AnCan virtual support group that meets four Wednesdays a month. I have found it very valuable and supportive in my journey.
From these men, I have come to realize that if active surveillance is pursued, you need to be involved with a Center of Excellence to monitor your situation. This is really what I wanted to do and realized I would need to travel as there is nothing close to where I live.
I began doing some looking on my own, trying to decide where to go. One of the moderators from the AnCan support group, Howard Wolinsky, assisted me with this task and told me if I was interested, he knew of a urologist in St. Louis that would be good.
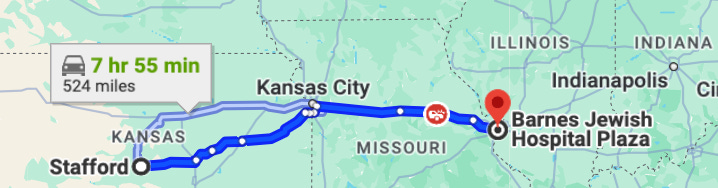
I decided that I would take Howard’s advice and contacted Dr. Gerald Andriole with Barnes Jewish Hospital and affiliated with Washington University. Dr. Andriole scheduled a time for a consult and also a 3T multi-parametric MRI. In March 2021, my wife and I traveled to St. Louis, a seven-hour drive, had the MRI completed and met with him.
Dr. Andriole, a former researcher at the National Cancer Institute, became my new urologist, and I felt I was with someone who was very in tune with the latest developments in prostate cancer and a proponent of active surveillance. He performed transperineal biopsies, which I felt would eventually replace many transrectal procedures, decreasing infections, and sepsis, allowing a better sampling of the prostate.
They were also using micro-ultrasound to guide during the transperineal biopsy. Micro-ultrasound is more powerful and shows much more detail than conventional ultrasounds. We have discussed this in the support group as it is a new tool and can complement an MRI. He suggested I have a repeat biopsy in November.
In October 2021, I received an email from Dr. Andriole that he would be leaving to take a job at Johns Hopkins. He recommended I continue my care with Dr. Arjun Sivaraman, who does most of their transperineal biopsies. In December of 2021, I traveled back to St. Louis for my biopsy. The procedure was done in an operating room under general anesthesia. It was a micro-ultrasound-guided transperineal biopsy. Dr. Sivaraman spoke with me after the procedure informing me that he did not see anything to target but took 12 cores. I received my pathology in a week and it was negative for any prostate cancer. I met virtually with him to review the report and he suggested I continue monitoring my PSA every 6 months and then we would meet virtually to review the results. My PSA fluctuated 2.2 to 3.3 over the next 18 months.
In May of 2023, I received a letter from Dr. Sivaraman stating that he would be leaving his practice at Washington University. I decided instead of beginning with another doctor in St. Louis, I would begin looking for one closer to home. I virtually interviewed a doctor from the Stephenson Cancer Center in Oklahoma City and one from the University of Kansas Cancer Center in Kansas City. I decided to go with Dr. William Parker from the University of Kansas Cancer Center.
Dr. Parker is a strong proponent of active surveillance and is receptive to my wishes but does prefer transrectal biopsies. However, he respects my decision to have a trans perineal biopsy (which they do perform) if it becomes necessary. This facility is about a 4-hour drive for me but also an opportunity to see and have some fun with the grandkids who live near there.
After reviewing my records, Dr. Parker suggested another MRI so on October 3rd, 2023, we headed to Kansas City and I had the MRI procedure. Two days later I met with Dr. Parker to review the results and it showed no lesions. We decided to continue monitoring my PSA every 6 months and if it remains stable, I will look to repeat another MRI in two years.
Dr. Parker suggested I should have another biopsy at that time but I want to see what my PSA and MRI results are. One comment that Dr. Parker made after initially reviewing my previous pathology and MRI results was, “You know, unfortunately, finding the small amount of cancer in your prostate was like finding a needle in a haystack. It has changed your life”
I do not totally consider this at all unfortunate. This experience has made me more health conscious and as a result, I’ve made some lifestyle changes with diet and exercise. I’ve also become associated with a great group of individuals who are dealing with their own journeys but are concerned with the well-being of others and helping wherever they can.
I am very appreciative of Howard and all of the other moderators and men involved in the AnCan support group. They have given me much information and support which impacted my journey and actually lifted some of the weight off of my shoulders. Each year that men can remain on active surveillance new information becomes available. Equipment and procedures become better.
More men with low-risk prostate cancer are electing active surveillance over unnecessary treatment and side effects. I feel those of us in rural areas are still going to have to travel distances to receive the care that we want. Many men in rural areas need to become better educated and aware of what is available. I have been talking to friends who are dealing with prostate cancer and passing along what I have learned.
My desire is that the medical community, especially urologists, would become aware of what is best for men with low-risk prostate cancer. Our quality of life is at stake!
Richard Brensing’s bio: “I am 67 years old and live in Stafford, Kansas, with my wife Shelly. We will have been married for 30 years in July. We are a blended family with five children. Three daughters from Shelly and one son and one daughter from me. From our five children, we are blessed with eleven grandchildren.
“I’m a fourth-generation farmer and have farmed for forty-two years but am in the process of retiring. I’ve been involved in the community serving on the local agricultural cooperative board, long-term care facility board. and Stafford Educational Foundation board.
“ I am very involved with my church, serving as an elder. As far as hobbies, I enjoy nature. I love to upland bird hunt and enjoy hunting with my son and sons-in-laws and now beginning to do so with the grandkids. Shelly and I also enjoy and look forward to traveling during our retirements and spending time with our grandkids.”
Part 2: Mighty hard row for medical migrant on AS: Hours and hours on the road, miles to go

(Editor’s note: In Part 1 of this series, I described the shortage of urologists especially in rural areas. Patients seeking Active Surveillance for low-risk cancers are medical migrants who have to drive long distances to get the care they need. 60% of U.S. counties don’t have a practicing urologist, and there are guarantees if they do that the urologi…
Chillax. It’s only perineural invasion.
Question: What is “perineural invasion”? Is it as scary as it sounds?
Dr. Zhou answers: In pathology reports, you may see a diagnosis of “perineural invasion” when prostate cancer is present. It describes that prostate cancer cells spread along and encircle nerves (See attached image)
. A large prostate cancer gland in the center tightly wraps around a nerve).
What does “perineural invasion” mean for patients’ outcomes and treatment?
Perineural invasion can be seen in both prostate biopsy and radical prostatectomy specimens.
The significance of finding it in the prostate biopsies has been studied extensively, but whether it indicates a worse outcome remains unclear.
More importantly, perineural invasion does not seem to have an impact on treatment.
For example, perineural invasion diagnosed in prostate biopsies should not prevent patients from receiving bilateral nerve-sparing radical prostatectomy. Similarly, the presence of perineural invasion should not exclude eligible patients from active surveillance. The caveat is that patients with perineural invasion in the prostate biopsy may have a greater risk of disease progression when on active surveillance and. therefore, patients may need closer follow-up. This information should be factored in the decision for active surveillance.
References:
1. De la Calle CM, et al. Clinical Significance of Perineural Invasion in Men With Grade Group 1 Prostate Cancer on Active Surveillance. J Urol. Vol. 209, 180-186, January 2023.
2. Niu, Y.; Förster, S.; Muders, M. The Role of Perineural Invasion in Prostate Cancer and Its Prognostic Significance. Cancers 2022, 14, 4065. https://doi.org/10.3390/cancers14174065
Dr. Zhou is the Chair and Pathologist-in-Chief of the Tufts Medical Center, and Professor and Chair of the Department of Anatomic and Clinical Pathology, Tufts University School of Medicine in Boston. He has published over 200 peer-reviewed articles and numerous book chapters and edited five textbooks of urological and prostate pathology. He is currently a member of the United States and Canadian Academy of Pathology Board of Directors, and the immediate past President of the Genitourinary Pathology Society (GUPS), an international organization for urological pathologists.
Please send questions to mailto:pros8canswers@gmail.com
Keep the questions short and sweet. They should be of general interest. Sign with your real name, or just initials, tell me where you live, how long you‘ve been on AS, how it’s going for for you. Share a whimsical signature if you’re so inclined.
For more on perineural invasion:
(Part II) The perineural invaders

(Editor’s note: Jeff Coleman and I were emailing the other day about something or other, and he mentioned his “roller coaster of emotions” with having been diagnosed with perineural invasion. I published Jeff’s story on Sunday. I told him I coincidentally was preparing an article on PNI, featuring an interview with Hopkins urologic oncology fellow, Cla…
ASPI webinar on how AI will decrease overdiagnosis and overtreatment of prostate cancer
By Howard Wolinsky
AI, short for artificial intelligence, is in the headlines increasingly. Medical care is expected to receive the biggest benefits in the field, including prostate cancer.
Join Active Surveillance Patients International (ASPI) on Feb. 24 at noon-1:30 p.m. Eastern to hear a panel talk about AI and how it will be affecting our lives as prostate cancer patients in a program entitled “How AI will decrease overdiagnosis and overtreatment of prostate cancer.”
The panel includes:
—Niels Olson, MD, is a board-certified pathologist and the Chief Medical Officer at the Defense Innovation Unit in Mountain View, California. In this role, he oversees research programs in machine learning/AI for a broad spectrum of anatomic pathology applications, augmented reality microscopy, and artificial intelligence applications in radiology.
—Bruno Barrey, a robotics engineer from suburban Detroit, who was able to avoid Androgen Deprivation Therapy because of an analysis by Artera AI as he transitioned from Active Surveillance to radiation treatment.
Send questions in advance to: mailto:pros8canswers@gmail.com, or just cut and paste pro8canswers@gmail.com
What’re you waiting for? Sign up for ZERO support group on AS in March
By Howard Wolinsky
For the past three years, I have run a special Active Surveillance support group for ZERO. Last year, our virtual support meeting drew 60 patients to talk about AS. By far, it was the biggest session of any at the annual ZERO Summit.
Be there or be square: 11 a.m. Eastern on March 12, 2024.
Register:
https://us02web.zoom.us/meeting/register/tZUsfuqgrjIoG9AWf7voMhzT_UjdqbQQbQPA